Context
Managed Care Fashions. For greater than three many years, states have elevated their reliance on managed care supply programs with the purpose of bettering entry to sure providers, enhancing care coordination and administration, and making future prices extra predictable. Throughout the states, there’s huge variation within the populations required to enroll in managed care, the providers coated (or “carved in”), and the quality and performance incentives and penalties employed. Most states contract with risk-based managed care organizations (MCOs) that cowl a complete set of advantages (acute care providers and typically long-term care), however many additionally contract with restricted profit pay as you go well being plans that provide a slender set of providers similar to dental care, non-emergency medical transportation, or behavioral well being providers. A minority of states function main care case administration (PCCM) applications which retain fee-for-service (FFS) reimbursements to suppliers however hyperlink enrollees with a main care supplier who’s paid a small month-to-month payment to supply case administration providers along with main care. Whereas the shift to MCOs has elevated price range predictability for states, the proof concerning the impression of managed care on entry to care and prices is each restricted and blended.5,6,7 In 2024, the Biden administration finalized main Medicaid managed care regulations designed to advance entry and promote high quality of look after enrollees. These guidelines are complicated and set to be applied over a number of years until overturned or delayed by Congress or the Trump administration.
Capitation Charges and Threat Mitigation. MCOs are at monetary threat for providers coated below their contracts, receiving a per member per month “capitation” fee for these providers. Capitation charges should be actuarially sound8 and are utilized prospectively, sometimes for a 12-month ranking interval, no matter adjustments in well being care prices or utilization.9 States might use quite a lot of risk mitigation tools to make sure funds are usually not too excessive or too low, together with threat sharing preparations, threat and acuity changes, medical loss ratios (MLR), or incentive and withhold preparations. When, nevertheless, important enrollment, utilization, value, and acuity adjustments started to emerge early within the COVID-19 public well being emergency, CMS allowed states to modify managed care contracts, and plenty of states applied COVID-19 associated “threat corridors” (the place states and well being plans conform to share revenue or losses), permitting for the recoupment of funds. States and plans confronted one other interval of heightened fee setting uncertainty when the continuous enrollment provision expired on March 31, 2023, leading to acuity and utilization shifts throughout the remaining inhabitants that had been tough to foretell.
Trying forward, the 2024 Medicaid managed care rule requires states to include all state directed funds (SDPs) via capitation fee setting changes as an alternative of utilizing “separate payment terms” (which offer funds exterior of base capitation charges) starting in July 2027.10 The 2025 federal price range reconciliation law (H.R.1) can even create fee setting challenges for states because the Medicaid provisions impacting enrollment and spending (e.g., work necessities, extra frequent eligibility redeterminations, and supplier tax and SDP caps and reductions) roll out over the following a number of years.
Prior Authorization and Synthetic Intelligence (AI). MCOs usually require sufferers to acquire approval of sure well being care providers or medicines earlier than the care is offered, an insurance coverage observe generally known as “prior authorization”. Subjecting a service or drug to prior authorization permits the MCO to judge whether or not the care is roofed, medically mandatory, and being delivered within the applicable setting, however may also enhance the executive burden on suppliers and typically delay or restrict entry to care. To scale back administrative prices and processing occasions and enhance consistency of selections, well being insurers are increasingly turning to AI to automate the processing of prior authorization requests. Utilizing AI for this objective, nevertheless, is drawing scrutiny as a consequence of considerations that poorly implemented AI can harm patients. In June 2025, the Division of Well being and Human Companies (HHS ) announced a voluntary initiative the place dozens of well being insurers pledged to scale back the burden of prior authorizations throughout insurance coverage markets, together with a dedication to develop “actual time” responses to digital prior authorization requests, which can contain rising the usage of AI. In July 2025, the Trump administration released an AI motion plan, emphasizing the removing of regulatory “purple tape” and enabling sooner adoption of AI instruments, and in 2026, the Administration plans to launch a new innovation mannequin to check the usage of applied sciences, together with AI and machine studying, within the prior authorization evaluate course of for choose Medicare providers. In September 2025, the launch of the Protected AI in Medicaid Alliance was announced, bringing collectively 32 states and business leaders to develop frameworks for AI adoption and use in state Medicaid applications.
This part offers details about:
- Managed care fashions
- MCO medical loss ratio (MLR) and remittance necessities
- Threat corridors
- MCO capitation fee amendments and fee setting challenges
- State oversight of MCO use of AI in prior authorization processes
Findings
Managed Care Fashions
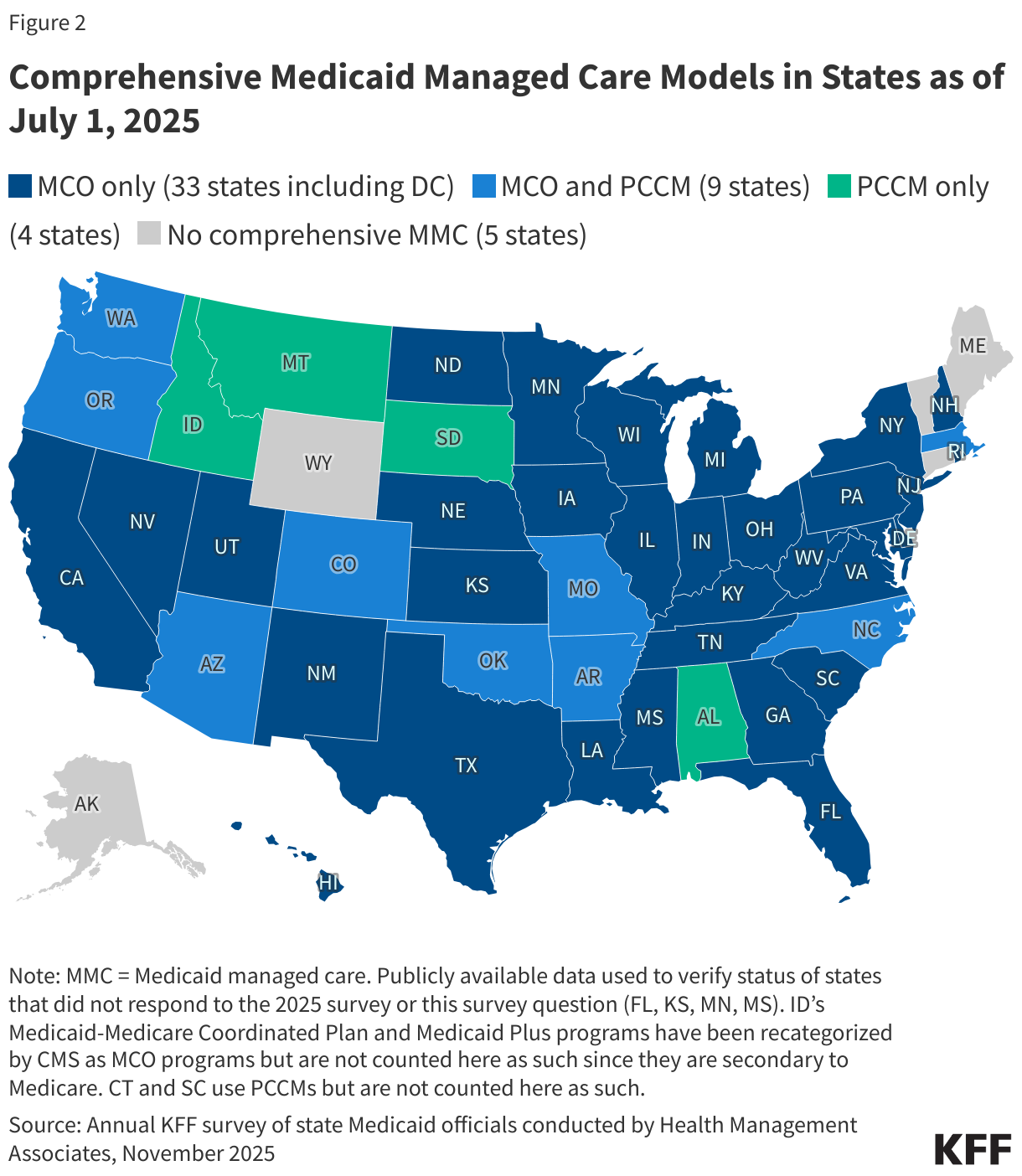
Capitated managed care stays the predominant supply system for Medicaid in most states. As of July 1, 2025, all states besides 5 – Alaska, Connecticut,11 Maine, Vermont,12 and Wyoming – had some type of managed care (MCOs and/or PCCM) in place (Determine 2). As of July 1, 2025, 42 states13 had been contracting with MCOs (unchanged from 2024); solely two of those states (Colorado and Nevada) didn’t supply MCOs statewide (though Nevada plans to develop MCOs statewide in 2026). 13 states reported working a PCCM program (with the addition of Missouri).14 Though not counted on this 12 months’s report, following the passage of HB 345, Idaho expects to finish its PCCM program by December 2025 and implement complete MCOs by January 2029.
Of the 46 states that function some type of complete managed care (MCOs and/or PCCM), 33 states function MCOs solely, 4 states function PCCM applications solely, and 9 states function each MCOs and a PCCM program. In complete, 28 states15 had been contracting with a number of restricted profit pay as you go well being plans (PHPs) to supply Medicaid advantages together with behavioral well being care, dental care, imaginative and prescient care, non-emergency medical transportation (NEMT), or long-term care (LTC).
Capitation Charges and Threat Mitigation
Minimal Medical Loss Ratios (MLRs) and Remittance Necessities
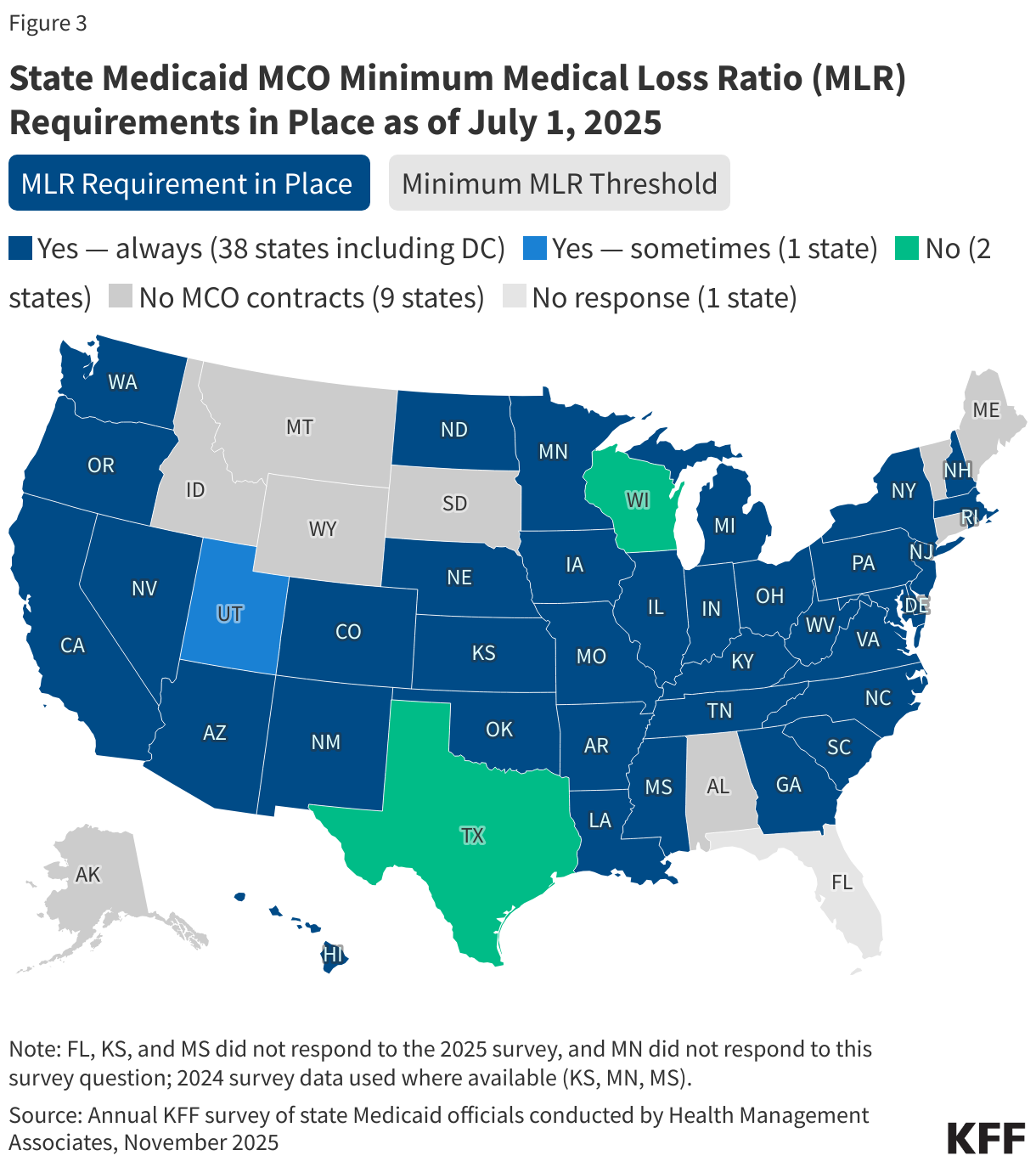
The MLR displays the proportion of complete capitation funds acquired by an MCO spent on scientific providers and high quality enchancment, the place the rest goes to administrative prices and earnings. To restrict the quantity that plans can spend on administration and maintain as revenue, CMS printed a final rule in 2016 that requires states to develop capitation charges for Medicaid to realize an MLR of not less than 85% within the fee 12 months.16 There is no such thing as a federal requirement for Medicaid plans to pay remittances to the state in the event that they fail to satisfy the MLR commonplace, however states have discretion to require remittances. The 2024 Consolidated Appropriations Act included a financial incentive to encourage sure states to gather remittances from Medicaid MCOs that don’t meet minimal MLR necessities. As state Medicaid applications confronted heightened uncertainty because of the COVID-19 pandemic (2020) and the unwinding of the pandemic-era steady enrollment provision (beginning in 2023), analysis of Medicaid managed care market knowledge (reported to the Nationwide Affiliation of Insurance coverage Commissioners) confirmed a lower within the common Medicaid MLR in 2020 – 2022 in contrast with prior years, adopted by a rise in 2023. More recent evaluation suggests the typical Medicaid MLR continued to extend in 2024. This 12 months’s survey requested states whether or not they have a state required minimal MLR and whether or not they require MCOs that don’t meet the minimal MLR requirement to pay remittances.
Almost all MCO responding states (38 of 41) reported a minimal MLR requirement is at all times in place for MCOs as of July 1, 2025 (Determine 3). Amongst responding states, responses had been unchanged/in line with last year’s survey. Whereas states should use plan-reported MLR knowledge to set future fee charges in order that plans will “moderately obtain” an MLR of not less than 85%, states are usually not required to set a minimal MLR for his or her managed care plans. If states set a minimal MLR requirement, it should be not less than 85%.17 Whereas most states that described their necessities reported a minimal MLR requirement of 85%, a number of states reported greater necessities that ranged from 86% to 93%. A number of states famous that minimal MLRs might differ by program or inhabitants. For instance, in Pennsylvania, the minimal MLR requirement is ready at 85% for MCOs masking acute care solely (hospital and doctor providers) and at 90% for MCOs that cowl acute care and LTC. Equally, New Jersey reported the minimal MLR requirement is ready at 85% for non-LTC populations and 90% for LTC populations coated below MCO contracts. In Indiana, the minimal MLR requirement is ready at 85% for MCOs that cowl youngsters and pregnant people, 87% for MCOs that cowl ACA enlargement adults, and 90% or greater for MCOs that cowl extra complicated populations similar to older adults (which may be receiving LTC) and folks with disabilities.
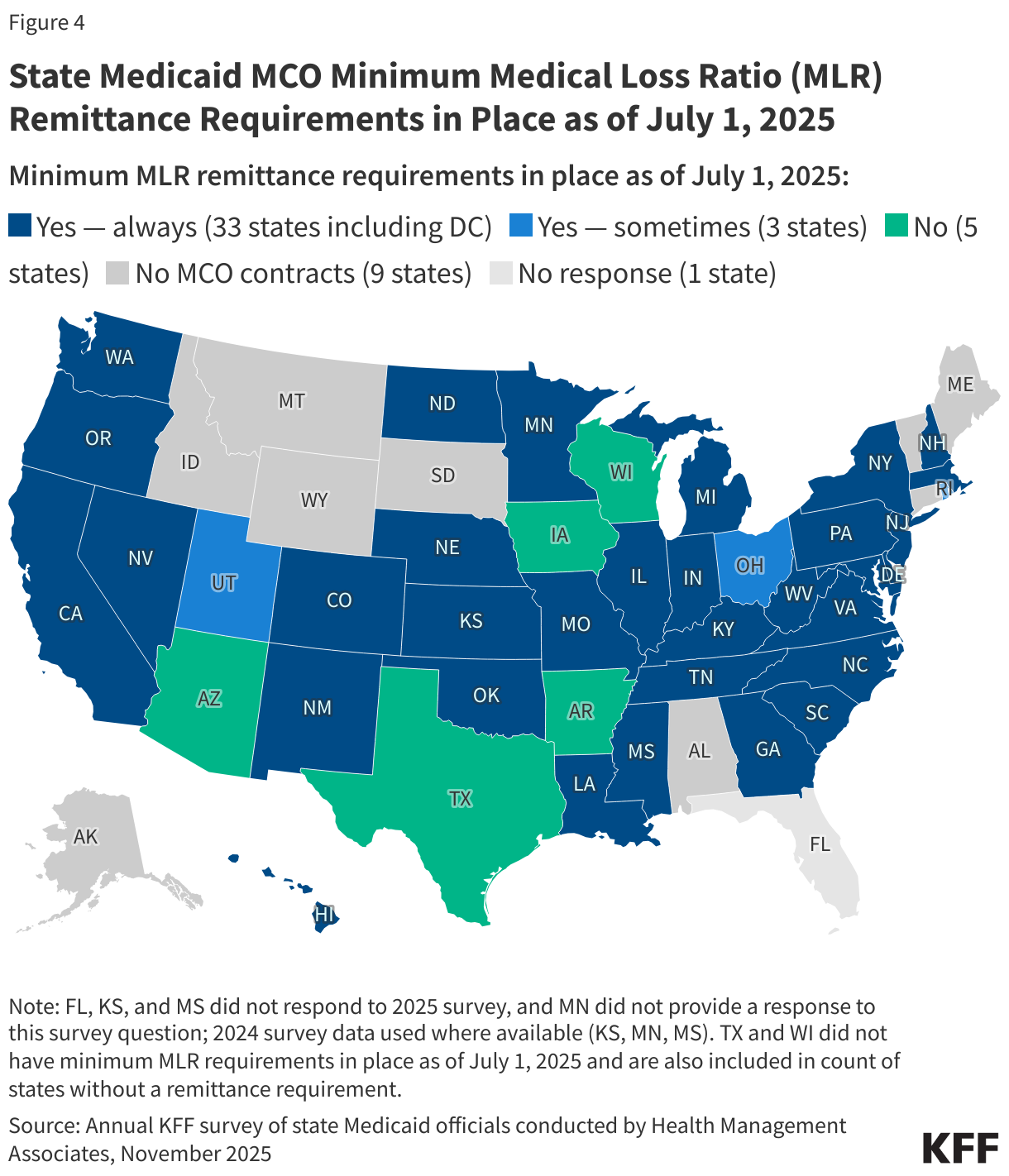
Greater than three-quarters of responding MCO states (33 of 41) report they at all times require remittance funds when an MCO doesn’t meet minimal MLR necessities (Determine 4). Thirty-three states reported that they at all times require MCOs to pay remittances, whereas three states indicated they often require MCOs to pay remittances (amongst responding states, responses had been usually in line with last year’s survey18). States reporting that they often require remittances might restrict this requirement to sure MCO contracts. For instance, Rhode Island reported that the remittance requirement didn’t apply to all populations.
Moreover, some states (North Carolina, Oregon, and Tennessee) give MCOs that fail to satisfy the state required minimal MLR the choice to both remit funds to the state and/or use funds in the direction of group reinvestments. California reported CMS requires its plans to cross MLR reporting and remittance necessities right down to risk-bearing subcontractors.19 5 states don’t require remittances (together with two states that don’t set a minimal MLR requirement). States that shouldn’t have minimal MLR and remittance necessities in place might produce other threat mitigation methods similar to revenue caps or expertise rebates and/or threat corridors.
Threat Corridors
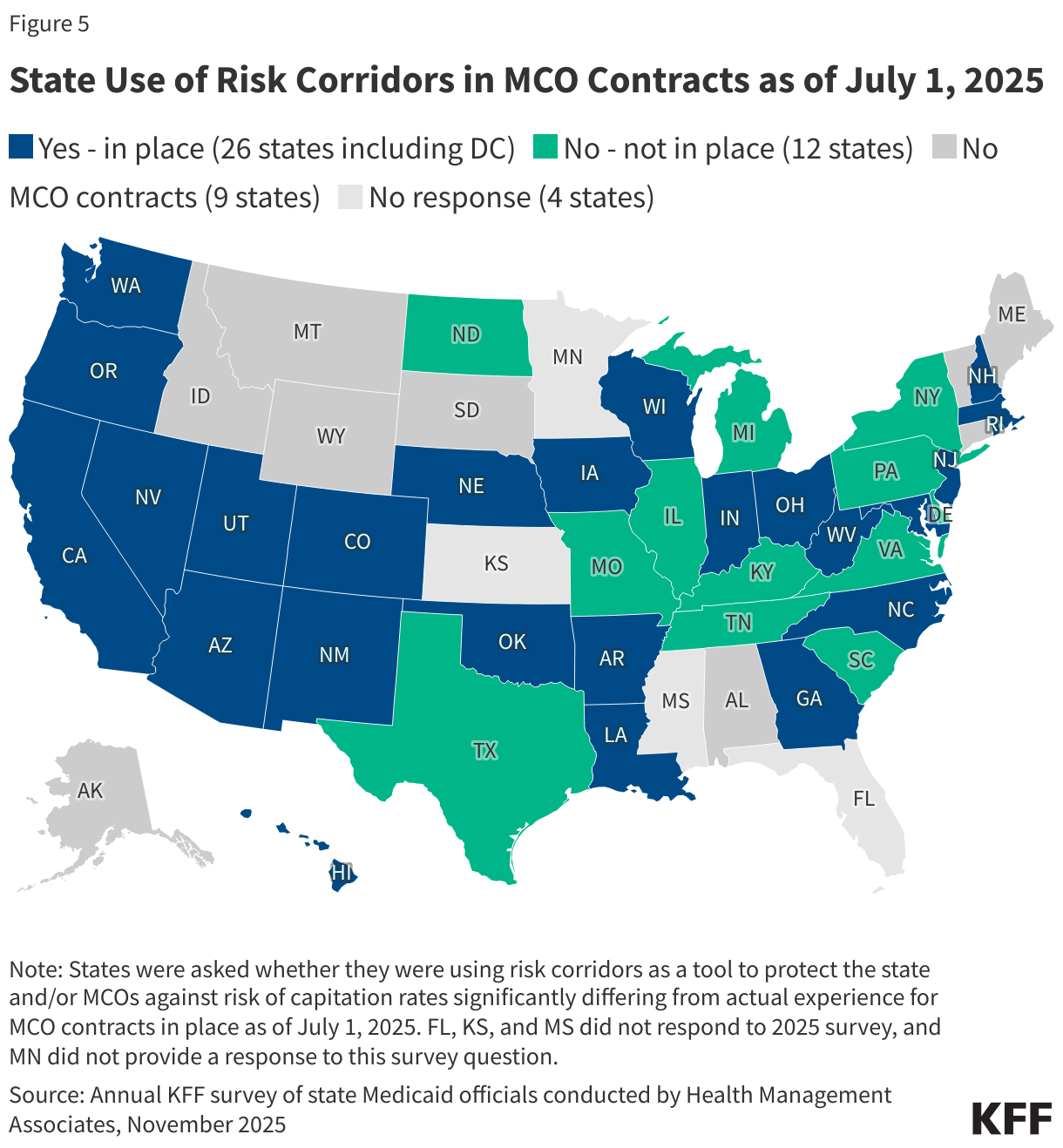
Risk corridors enable states and well being plans to share revenue or losses (at percentages laid out in plan contracts) if mixture spending falls above or under specified thresholds. Below two-sided threat corridors, states and plans might share in plan earnings and losses. Though much less widespread, some states might use “one-sided” threat corridors that apply solely to earnings or losses. Threat hall thresholds could also be tied to a goal MLR. Threat corridors might cowl all/most medical providers (and enrollees) below a contract or could also be extra narrowly outlined, masking a subset of providers or enrollees. States might introduce threat corridors on a time-limited foundation—for instance, following the enlargement of protection to new teams (e.g., ACA Medicaid enlargement adults). CMS inspired states to implement two-sided risk mitigation strategies, together with threat corridors, for ranking intervals impacted by the COVID-19 public well being emergency. In 2023, nearly two-thirds of responding MCO states reported implementing a pandemic-related MCO threat hall (in 2020, 2021, and/or 2022), resulting in the recoupment of funds for a lot of states. On this 12 months’s survey, states had been requested whether or not they had been utilizing threat corridors as a device to guard the state and/or MCOs towards threat of capitation charges considerably differing from precise expertise for MCO contracts in place as of July 1, 2025.
Over two-thirds of responding MCO states (26 of 38) reported utilizing threat corridors for MCO contracts in place as of July 1, 2025 (Determine 5).20 Among the threat corridors that states described broadly apply to all/most populations and/or prices whereas different threat corridors apply to particular populations and/or a subset of prices. States ceaselessly reported the usage of a number of threat corridors. For instance, Arizona reported utilizing a two-sided medical threat hall (for all applications) which incorporates profit prices however excludes administrative prices and a two-sided threat hall for fastened administrative prices for its largest program with probably the most inhabitants fluctuation (to make sure fastened prices are coated no matter inhabitants fluctuations). California reported a number of threat corridors together with a two-sided threat hall for its new Enhanced Case Administration (ECM) profit, noting the potential variability (e.g., by plan and area) related to the implementation and ramp up of ECM helps; a two-sided threat hall for state directed supplemental funds for family planning services; and a two-sided threat hall for a brand new federally certified well being middle various fee mannequin (APM) program. Whereas nearly all of threat corridors described by states are two-sided, not less than three states (Nebraska, Washington, and West Virginia) reported utilizing one-sided threat corridors for not less than sure populations or MCO applications.
Price Amendments and Price Setting Challenges
State Medicaid applications use the newest and correct enrollment, value, and utilization knowledge accessible to make sure that MCO capitation charges are actuarially sound and that MCOs are usually not over-paid or under-paid for the providers they ship. Even when risk mitigation methods are in place (e.g., MLR with remittance and/or threat corridors), states might decide fee amendments are mandatory, for instance, if their precise expertise differs considerably from the assumptions used for the preliminary licensed charges. Throughout a contract rating period, states might enhance or lower charges by 1.5% per fee cell (which apply to inhabitants subgroups with a number of widespread traits similar to age, gender, eligibility class, and geographic area) with out looking for CMS approval for the change (completely different guidelines apply for states with authorised fee ranges per cell).21 To make a bigger change, states should submit a fee modification for federal approval that addresses and accounts for all variations from probably the most not too long ago licensed charges.
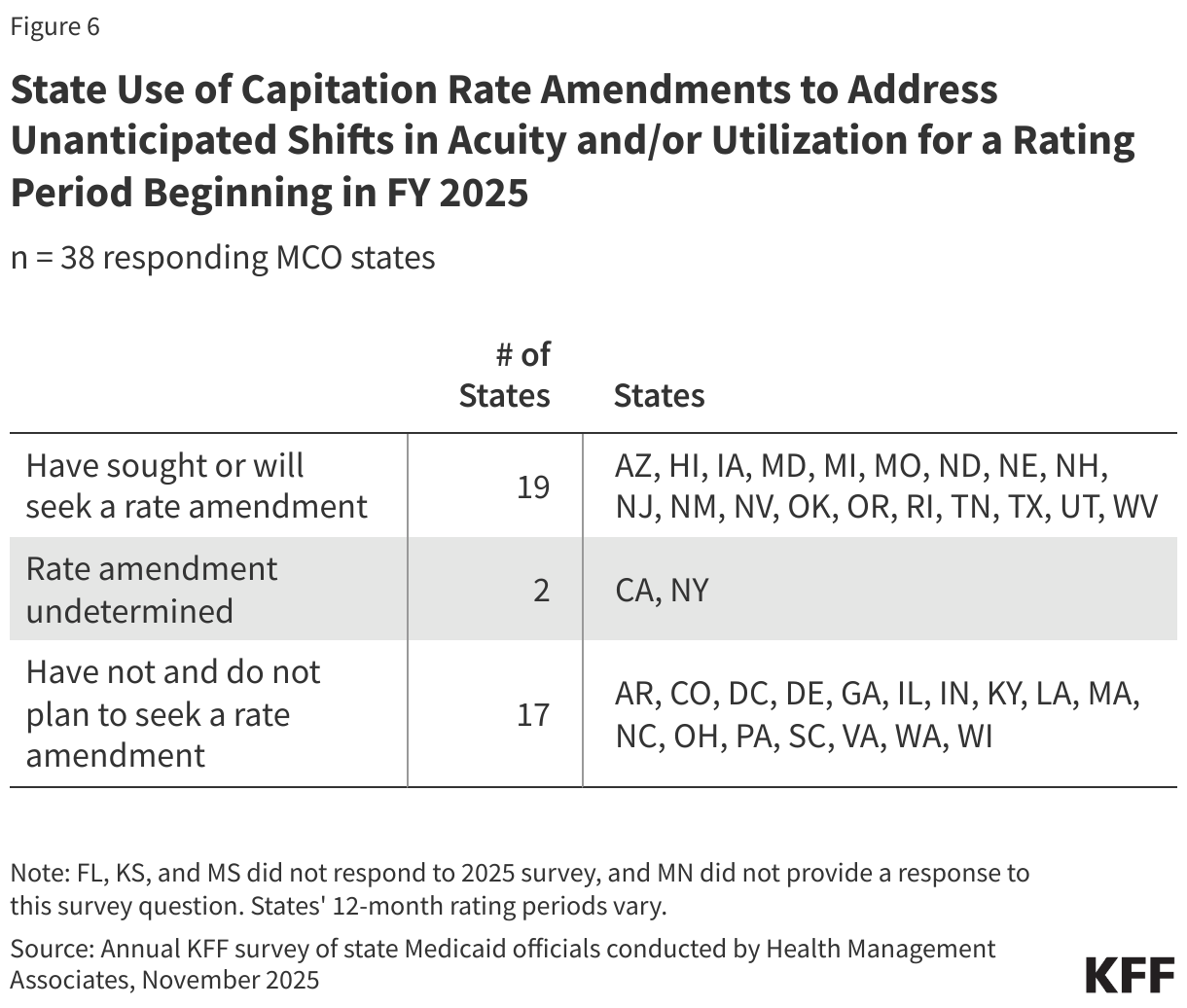
Through the unwinding of the pandemic-era Medicaid steady enrollment provision, thousands and thousands of individuals were disenrolled and states and plans confronted appreciable fee setting uncertainty. Greater member threat and utilization patterns started to emerge by late 2023, and plenty of states sought federal approval to regulate charges to handle these shifts in FY 2024. This 12 months’s survey requested states whether or not they have or will search CMS approval for a capitation fee modification to licensed charges to handle unanticipated shifts in acuity and/or utilization within the ranking interval that started in FY 2025.
Half of responding MCO states (19 of 38) reported looking for CMS approval for a capitation fee modification to handle unanticipated shifts in acuity and/or utilization for a ranking interval starting in FY 2025 (Determine 6). Of the 19 states that reported looking for fee amendments, almost all reported that the modification(s) resulted in a rise to capitation charges and about two-thirds reported that the adjustments utilized retrospectively (i.e., adjusted capitation charges for a interval that already handed).
Through the unwinding interval, state actuaries used quite a lot of approaches to account for adjustments in value, utilization, and member acuity.22 This 12 months’s survey included questions to higher perceive capitation fee setting challenges within the post-unwinding setting. Some states famous making important adjustments to the method for growing actuarially sound capitation charges post-unwinding, together with the incorporation of acuity changes and mid-year critiques of charges to find out if adjustments are applicable.
Most responding MCO states reported experiencing or anticipating to expertise new or notable challenges setting capitation charges for ranking interval(s) that start in FY 2026. Many of those states reported challenges as a consequence of greater acuity and utilization developments. Some states reported challenges with projecting future pharmacy developments and prices. A number of states additionally talked about rising medical prices (e.g., inpatient hospital prices) in addition to state budgetary pressures and uncertainty. Many states anticipate challenges with projecting potential impacts of federal coverage adjustments efficient after FY 2026. This consists of work necessities and extra frequent eligibility redeterminations for enlargement adults below the not too long ago handed reconciliation law, which has implications for member enrollment and acuity (on common). A number of states additionally talked about challenges with calculating SDPs stemming from regulatory adjustments (e.g., the 2024 managed care rule’s prohibition on separate phrases), and some states talked about uncertainty concerning the reconciliation legislation’s limits on SDPs.
Prior Authorization and Synthetic Intelligence (AI)
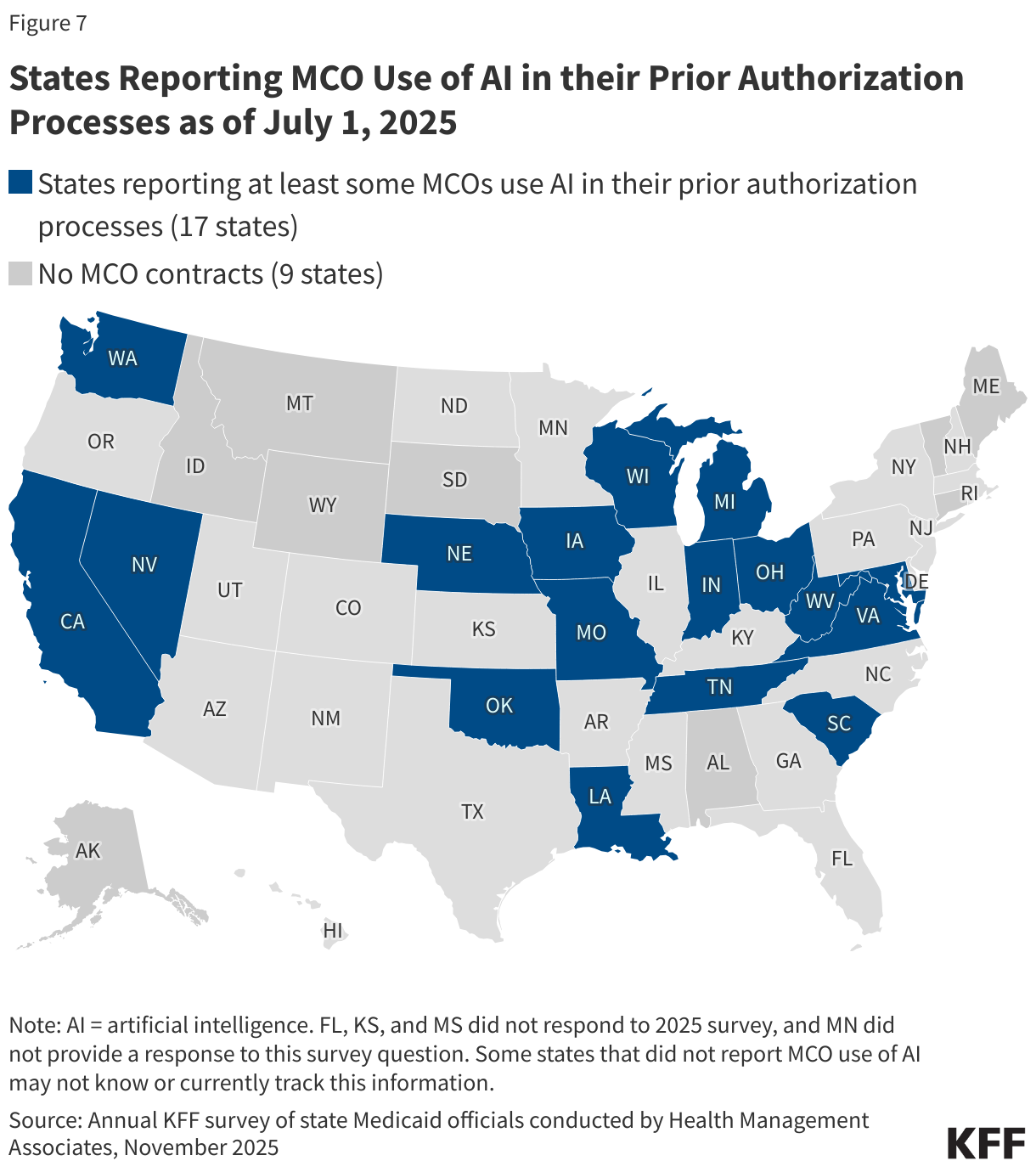
Whereas well being insurers are increasingly using AI to automate components of the prior authorization course of, there’s restricted data accessible about its use and impression inside Medicaid managed care. The Medicaid and CHIP Fee And Entry Fee (MACPAC) discovered that whereas there are potential advantages of automation in prior authorization similar to administrative efficiencies and sooner processing occasions, it could additionally pose potential dangers or challenges relying on how it’s administered and monitored. Within the absence of complete federal coverage governing AI use and oversight in prior authorization, some states have taken steps to manage or monitor use of AI by well being plans. A November 2024 report from the Nationwide Affiliation of Insurance coverage Commissioners highlighted that transparency to customers, suppliers, and regulators is a vital element of AI oversight. This 12 months’s survey requested states whether or not the MCOs with which they contract use AI of their prior authorization processes as of July 1, 2025.23
Almost half of responding MCO states (17 of 38) reported data of not less than a few of the MCOs with which they contract utilizing AI of their prior authorization processes as of July 1, 2025 (Determine 7). Not less than two states (Oklahoma and South Carolina) reported that AI is used just for prior authorization approvals (vs. use for denials/opposed determinations). Some states that didn’t report MCO utilization of AI might not know or presently observe this data.
Lower than one-quarter of responding MCO states (7 of 38) reported requiring MCOs to reveal the usage of AI in prior authorization processes. States had been requested in the event that they require MCOs to reveal the usage of AI in prior authorization processes (to the state Medicaid company, enrollees, and/or suppliers) as of July 1, 2025. Seven states (California, District of Columbia, Georgia, Indiana, Nebraska, Tennessee, and Virginia) reported requiring disclosure to the state Medicaid company. 5 of these states (District of Columbia, Indiana, Nebraska, Tennessee, and Virginia) indicated MCOs should submit a request to make use of AI to the state expertise officer or Medicaid company for evaluate earlier than implementation. Three states (California, Georgia, and Indiana) reported requiring disclosure to enrollees and suppliers.
State examples of AI disclosure necessities embody:
- In California, MCOs are required to reveal the use and oversight of AI instruments of their written utilization administration insurance policies and procedures. These paperwork should be made accessible to suppliers, enrollees, and the general public upon request.
- Indiana has adopted an AI coverage governing the usage of AI applied sciences throughout all state companies. In alignment with this coverage, the state Medicaid company requires plans to submit any AI instruments or programs for formal evaluate. Indiana’s State Company AI Techniques Commonplace requires MCOs to conduct a readiness evaluation previous to implementation or use of any AI device or system in addition to annual follow-up or advert hoc assessments when important adjustments are made to the AI device.
- In Tennessee, MCOs are required to contact the state Medicaid company’s AI Governance Committee when the usage of AI is contemplated in any capability. MCOs should share what vendor is being thought-about, what objective the AI is serving, how outputs are being verified, what system dangers and vulnerabilities exist, and the way knowledge is being safeguarded.
Many states reported considerations and challenges with the usage of AI in MCO prior authorization processes. When requested to explain their prime considerations or challenges (if any) with the usage of AI in MCO prior authorization processes, states ceaselessly cited potential for bias, improper denials, privateness and safety dangers, and insufficient human/clinician oversight. Some states additionally reported considerations with making certain compliance with federal and state necessities, complexities associated to oversight, and transparency of AI decision-making processes.
A number of states reported implementing new or expanded oversight actions or adopting different safeguards in FY 2025 or 2026 to help applicable use of AI in MCO prior authorization processes. For instance, 5 states (California, Maryland, Nevada, New Hampshire, and Ohio) reported introducing or plans to introduce language in MCO contracts concerning the usage of AI. Texas reported working to develop an ordinary course of to evaluate MCO AI instruments previous to implementation.