
Enrollment in Medicare Benefit, the personal plan various to conventional Medicare, has elevated steadily over time. The expansion in enrollment has been accompanied by a rise within the variety of Medicare Benefit plans, with the common beneficiary having the choice to decide on amongst 42 plans in 2025, together with 34 with prescription drug protection. Most Medicare Benefit insurers use supplier networks, together with different instruments, equivalent to prior authorization, to assist handle utilization and decrease prices. Whereas these practices could contribute to insurers’ means to supply extra benefits and scale back price sharing, they might additionally impose barriers to care by proscribing alternative of physicians, hospitals, and different suppliers, introducing extra complexity in evaluating and selecting plans, and creating potential for disruption in care preparations for sufferers when their hospitals and physicians are now not in-network.
Regardless of the wide selection of Medicare protection choices out there, there are restricted decision-support instruments for beneficiaries wishing to check Medicare Benefit supplier networks to one another and to conventional Medicare. Whereas Medicare beneficiaries say that physician availability is an important factor in choosing their protection, it may be difficult to evaluate which physicians are in-network throughout all out there plans. In 2025, as with prior years, the Medicare Plan Finder didn’t embody Medicare Benefit supplier community info. Beneficiaries have been directed to every plan’s web site to acquire details about the supplier community, and usually, the community directories aren’t out there in a uniform, easy-to-compare format. Additional compounding the issue, these directories are sometimes inaccurate. As of October 2025, prematurely of the 2026 plan yr, CMS will post supplier listing info on the Plan Finder utilizing info aggregated by a 3rd occasion, and beginning in 2027, Medicare Benefit insurers can be required to submit supplier info on to CMS for publication on-line.
To grasp how a lot supplier networks differ throughout Medicare Benefit plans, this transient examines the share of physicians out there to Medicare Benefit enrollees as a share of physicians out there to conventional Medicare beneficiaries, by county, plan traits, and doctor specialties, utilizing 2022 Medicare Benefit supplier directories. (See Strategies.) The evaluation finds broad variation in community breadth throughout plans and in comparison with conventional Medicare The scale of a Medicare Benefit plan’s community doesn’t essentially point out whether or not it contains sufficient physicians with the correct experience who can be found when sufferers want care, or whether or not these physicians are accepting new sufferers, although smaller networks improve the possibilities that enrollees pay extra for going out of network or expertise some disruption of their care preparations.
Key Findings:
- Medicare Benefit enrollees had been in a plan that included just below half (48%) of all physicians out there to conventional Medicare beneficiaries of their space in 2022, on common. Narrower networks restrict which docs, specialists, and different well being care suppliers can be found to Medicare Benefit enrollees, except they’re prepared and in a position to pay extra to go out-of-network. Narrower networks may also be disruptive for sufferers who want to change docs or hospitals to remain throughout the community for his or her care.
- For the one-fifth of Medicare Benefit enrollees in plans with the narrowest community, two out of three physicians out there to beneficiaries in conventional Medicare of their space had been out-of-network.
- Conversely, for the one-fifth of Medicare Benefit enrollees in plans with the broadest networks, fewer than one-third of physicians out there to conventional Medicare beneficiaries had been out of their plan’s community.
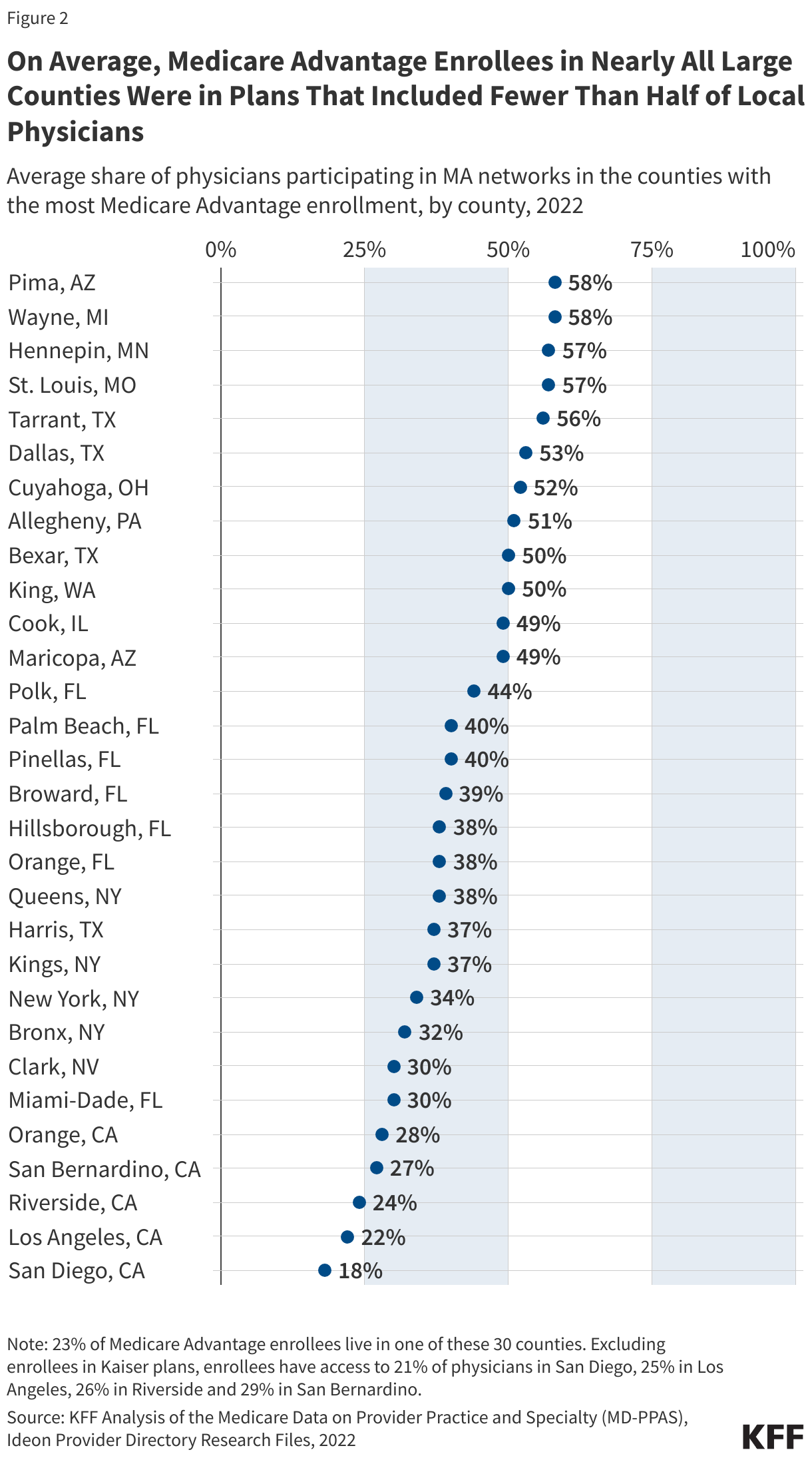
- The breadth of Medicare Benefit networks various broadly throughout counties. Among the many 30 counties with the biggest Medicare Benefit enrollment, the share of physicians out there to Medicare Benefit enrollees as a share of physicians out there to conventional Medicare beneficiaries ranged from a mean of 18% in San Diego, CA to a mean of 58% in Pima, AZ (Tucson). This variation throughout geographic areas implies that some Medicare Benefit enrollees have extra alternative amongst well being care suppliers than others.
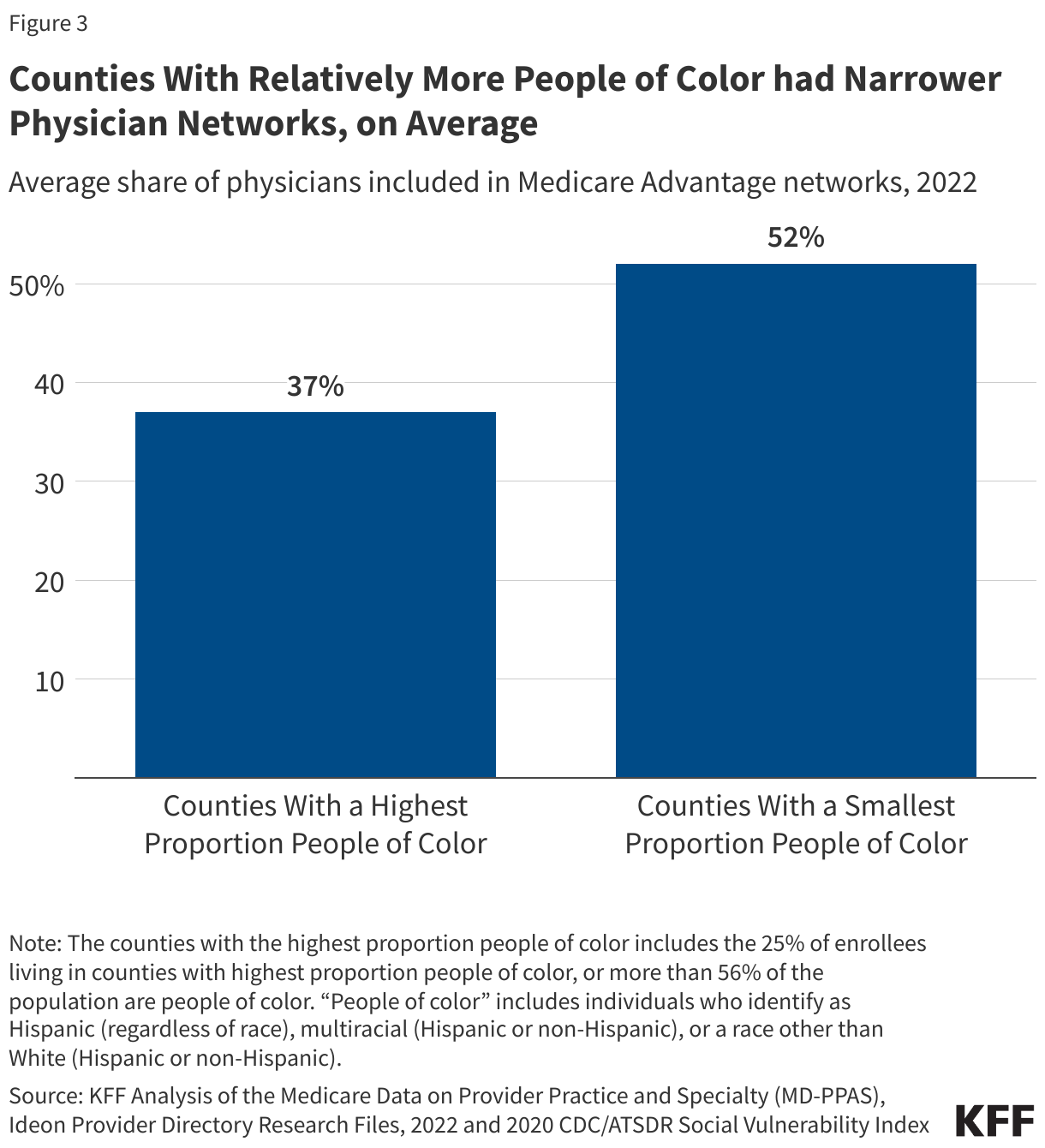
- In counties the place bigger shares of the inhabitants had been folks of shade, a smaller share of physicians out there to conventional Medicare beneficiaries had been in-network, on common, than in different counties (37% vs 52%).
- Even throughout the similar county, doctor networks typically various broadly throughout plans. One third (32%) of all Medicare beneficiaries lived in a county the place not less than one plan had lower than one-quarter of physicians out there to conventional Medicare beneficiaries and not less than one plan included not less than two-thirds of physicians out there to conventional Medicare beneficiaries, although these variations are troublesome for beneficiaries to decipher and never apparent when potential enrollees are evaluating their Medicare protection choices.
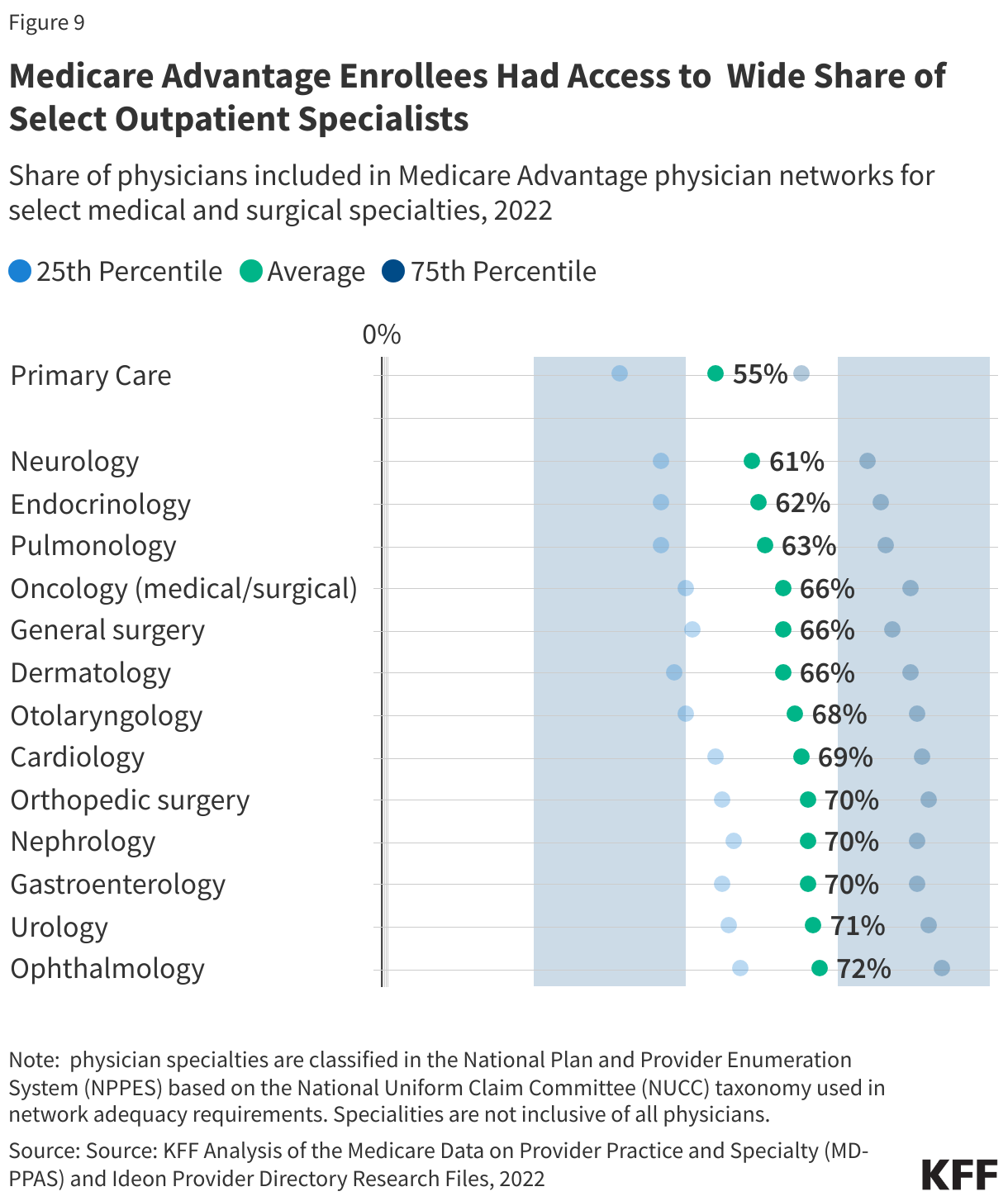
- The share of physicians out there to Medicare Benefit enrollees various by specialty. Typically, bigger shares of outpatient medical and surgical specialists had been in plan networks than main care physicians, with as many as 72% of ophthalmologists out there to conventional Medicare beneficiaries in plan networks in comparison with solely 55% of main care physicians, on common.
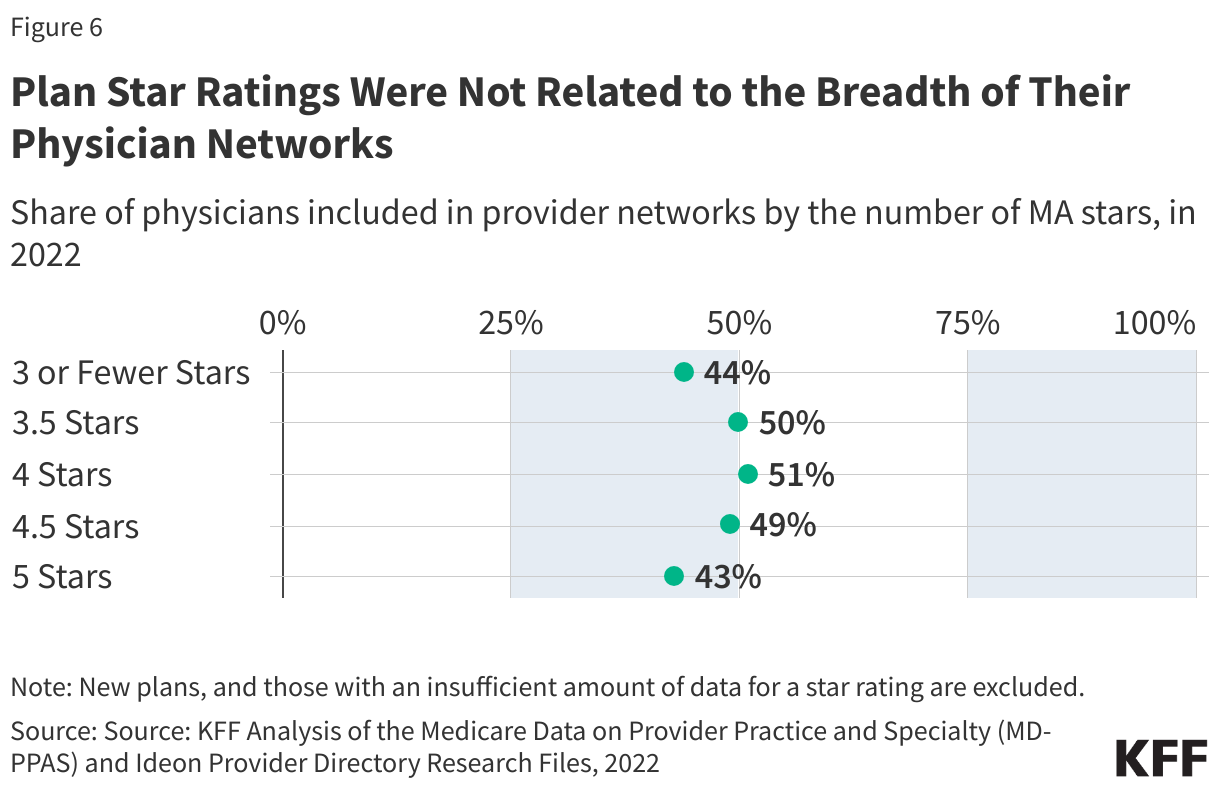
- Medicare Benefit plan high quality star scores weren’t correlated with the breadth of the doctor community. Although star scores had been supposed to assist beneficiaries select a plan that greatest meets their wants, they don’t convey the knowledge wanted for potential enrollees who prioritize the breadth of the supplier community.
Medicare Benefit Enrollees had Entry to About Half of the Physicians Obtainable to Conventional Medicare Beneficiaries.
Conventional Medicare beneficiaries might even see any doctor who participates in Medicare, so long as the doctor is taking new sufferers. Based on a separate KFF evaluation, just 1% of non-pediatric physicians have formally opted out of the Medicare program nationwide, and the vast majority of office-based physicians settle for new Medicare sufferers. In distinction, enrollees in Medicare Benefit should see suppliers who take part of their plan’s community or probably pay increased cost-sharing. On common, Medicare Benefit enrollees had been in a plan that included about half (48%) of physicians out there to conventional Medicare beneficiaries of their space in 2022 (Determine 1).
Some physicians are considerably much less more likely to take part in a Medicare Benefit community, equivalent to hospital-based emergency drugs docs and anesthesiologists. When these suppliers ship sure providers, equivalent to care in an emergency room or anesthesia throughout surgical procedure at an in-network facility, sufferers is not going to be liable for added prices as a result of the physician is out-of-network. If hospital-based physicians are excluded from the evaluation, the share of physicians out there to conventional Medicare beneficiaries who take part in Medicare Benefit networks will increase to 62%, on common. This evaluation considers all individual-level physicians who billed conventional Medicare, together with hospital-based physicians. Primarily based on out there knowledge just isn’t doable to determine which physicians, beneath what circumstances, wouldn’t result in increased prices for sufferers if the doctor had been out-of-network.
Many Medicare Benefit enrollees had been in plans with narrower networks that included considerably fewer physicians. One in 5 Medicare Benefit enrollees had been in plans with 32% or fewer of the physicians serving conventional Medicare beneficiaries. Which means for these Medicare Benefit enrollees, greater than two out of three physicians out there to conventional Medicare beneficiaries had been out-of-network. On the similar time, many Medicare Benefit enrollees had been in plans with broader networks, with one in 5 Medicare Benefit enrollees in plans that included not less than 63% of the physicians out there to conventional Medicare (Determine 1).

The share of physicians included in Medicare Benefit plan networks various broadly throughout counties.
Medicare Benefit plans are provided on the county stage. Like different traits of the Medicare Benefit market, equivalent to plan availability, the common breadth of Medicare Benefit plan networks various broadly throughout counties, starting from a mean of simply 15% of physicians out there to conventional Medicare beneficiaries in Charles County, MD (exterior Washington, D.C.) to 88% of physicians out there to conventional Medicare beneficiaries in Redwood, MN (in southern Minnesota).
Among the many 30 counties with the biggest Medicare Benefit enrollment, the share of physicians included in plan networks ranged from a mean of 18% in San Diego, CA, to a mean of 58% in Pima, AZ (Tucson).
Simply 30 counties are house to greater than 20% of all Medicare Benefit enrollees. In these counties, the share of physicians out there to conventional Medicare beneficiaries included in plan networks ranged from a mean of 18% in San Diego, CA to 58% in Pima, AZ (Tucson). A minimum of half of physicians had been in-network in simply 10 of those 30 counties. Conversely, in 20 of those 30 counties, fewer than half of all physicians out there to conventional Medicare beneficiaries had been in-network for Medicare Benefit enrollees, on common (Determine 2).
Counties with comparatively bigger populations of individuals of shade had smaller Medicare Benefit networks, on common
Medicare Benefit enrolls Black, Hispanic, and Asian and Pacific Islander Medicare beneficiaries at increased charges than White Medicare beneficiaries. Throughout dozens of measures examined in the literature, folks of shade, significantly Black Medicare Benefit enrollees, typically fare worse than White Medicare Benefit enrollees.
Plans in counties with a disproportionate share of residents who’re folks of shade tended to have narrower networks. Extra particularly, Medicare Benefit enrollees dwelling in counties with the biggest share of individuals of shade had entry to simply 37% of the physicians out there to conventional Medicare beneficiaries, on common, in contrast with 52% in counties the place folks of shade made up a smaller share of the inhabitants (Determine 3).
The differential entry to physicians persists when trying solely inside metropolitan counties (36% vs. 51%), which have narrower networks on common (see under) and sometimes bigger populations of individuals of shade.
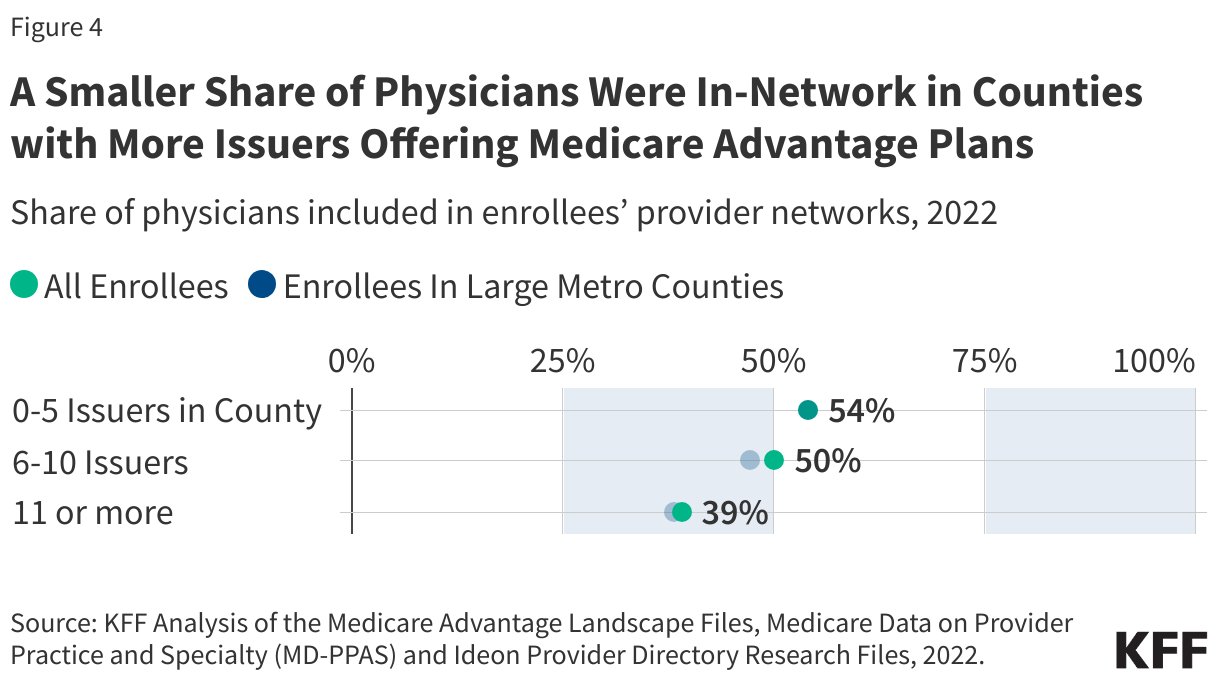
Counties with a bigger variety of insurers had smaller doctor networks, on common.
In 2022, the common Medicare beneficiary may select from plans provided by 9 companies, and one-quarter of beneficiaries had entry to plans from 11 or extra companies. On common, Medicare Benefit enrollees in counties the place extra companies provided plans had been in plans with smaller networks. Particularly, Medicare Benefit enrollees in counties with 11 or extra companies had been in plans that included lower than 4 in 10 (39%) physicians out there to conventional Medicare beneficiaries within the space, in comparison with 54% amongst Medicare Benefit enrollees in counties with 5 or fewer companies (Determine 4). The share of physicians who had been in-network on common was comparable when analyzing all Medicare Benefit enrollees and simply these in giant counties.
In rural counties, greater than half (53%) of physicians out there to conventional Medicare beneficiaries had been in-network, on common, barely greater than the nationwide common.
A larger share of Medicare beneficiaries dwelling in rural areas get their Medicare protection via conventional Medicare fairly than Medicare Benefit, although enrollment in Medicare Benefit has grown considerably in rural areas lately. On common, Medicare Benefit enrollees in rural areas have a barely bigger share of physicians out there to conventional Medicare beneficiaries within the community than these in metropolitan areas, 53% in contrast with 47%. A considerably smaller share of physicians follow in rural areas than in metropolitan areas, so broader networks in rural areas could not translate into higher entry to physicians.
The scale of doctor networks various broadly inside most counties.
Most Medicare beneficiaries can select from dozens of Medicare Benefit plans provided of their county. The plans differ throughout many dimensions, equivalent to premiums, price sharing, out-of-pocket limits, prescription drug protection, use of prior authorization, and the provision and generosity of advantages for non-Medicare coated providers. Moreover, the breadth of doctor networks varies broadly.
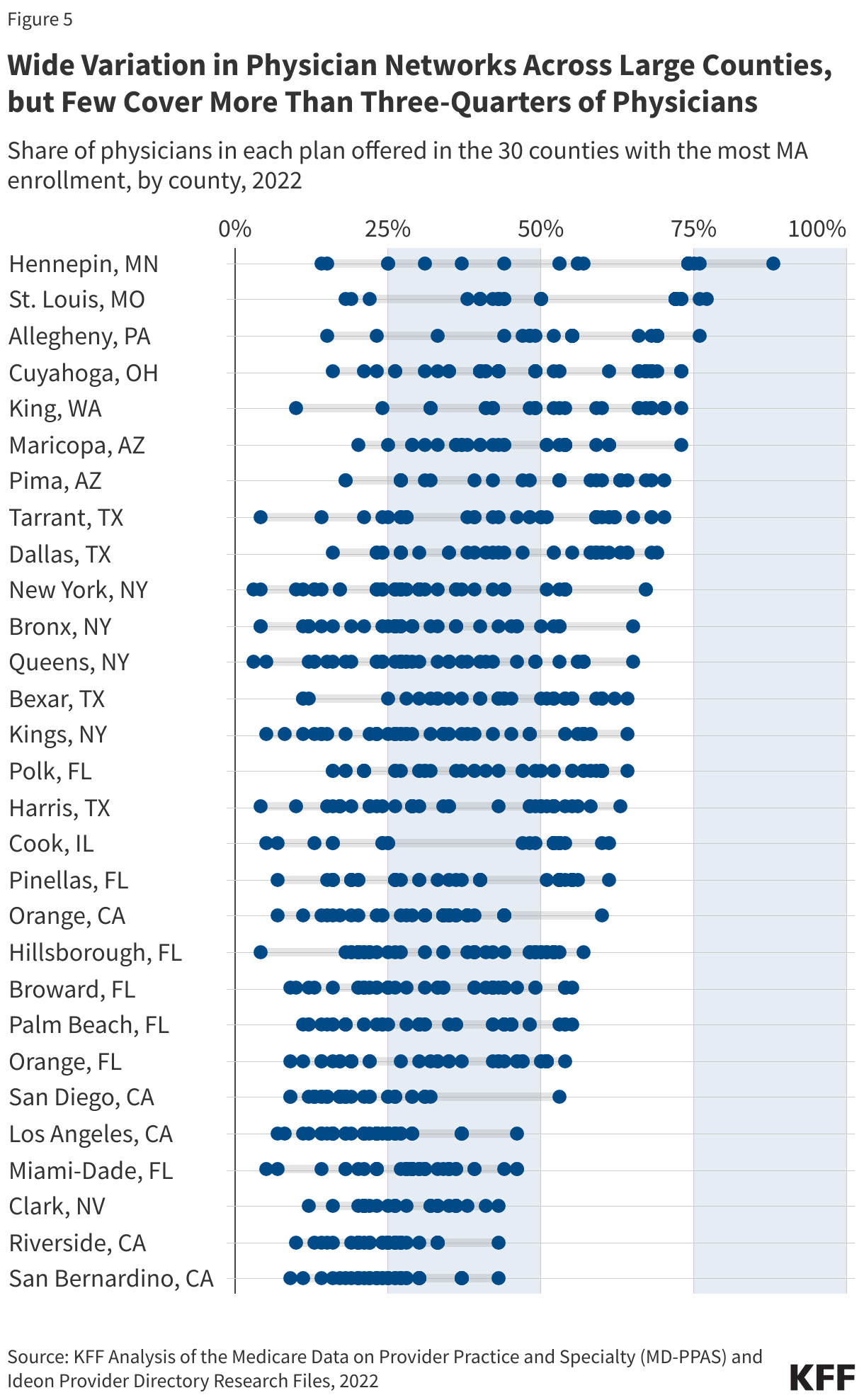
Practically two-thirds of Medicare Benefit enrollees lived in a county with not less than one plan that had fewer than 25% of physicians out there to conventional Medicare beneficiaries in-network and, conversely, not less than one plan with almost two-thirds (64%) of the physicians out there to conventional Medicare beneficiaries in-network. Such a big variation within the breadth of doctor networks implies that plan alternative has substantial implications for which docs somebody can see with out incurring extra cost-sharing.
Determine 5 reveals the share of physicians out there to conventional Medicare beneficiaries who’re in community for plans provided within the 30 counties with the biggest Medicare Benefit enrollment (which represents 23% of all Medicare Benefit enrollment). For instance, in Hennepin County, MN (which incorporates Minneapolis), the share of physicians out there to conventional Medicare beneficiaries who had been in community ranged from 14% to 88%. In Clark County, NV (which incorporates Las Vegas) the distinction throughout plans was smaller, however nonetheless substantial, starting from 12% to 43%.
Some docs didn’t take part in any Medicare Benefit plan community. On common, roughly 1 in 7 (14%) physicians who submitted Medicare claims weren’t included in any Medicare Benefit plan community. A big share of the docs who don’t take part in any Medicare Benefit community are hospital-based physicians, equivalent to emergency drugs docs and anesthesiologists (21% and 19% of all physicians who aren’t in any Medicare Benefit community, respectively). Whereas acquiring care from a non-network supplier typically leads to increased prices for sufferers, that’s not at all times the case. Particularly, emergency care is roofed whatever the supplier’s community standing. Moreover, sufferers are protected towards out-of-network expenses for sure providers offered throughout a hospital keep or process that happens in a hospital setting, when particular circumstances are met, equivalent to when the power or main supplier (e.g., a surgeon) is in community. In any other case, beneficiaries who see different sorts of physicians who aren’t in any Medicare Benefit plan community would both pay extra to keep up continuity of care or have to discover a new physician.
There have been variations within the measurement of Medicare Benefit networks throughout some Medicare Benefit plan traits, however not others.
Medicare Benefit plans with high-quality star scores didn’t have bigger doctor networks.
One of many items of knowledge that Medicare beneficiaries have when choosing a plan is the standard star score. Medicare Benefit plans are rated on a scale of 1-to-5 stars, which replicate efficiency on a big set of indicators, together with customer support, client satisfaction, the share of enrollees who obtain vaccines and screenings, and administration of sure circumstances, amongst others. Each plan availability and enrollment are skewed in the direction of plans with increased stars, with greater than 80% of enrollees on this evaluation in a plan with not less than 4 stars in 2022.
On common, enrollees in plans with 4.5 or 5 stars had a community that included 49% and 43% of physicians out there to conventional Medicare beneficiaries, respectively, in comparison with 51% for plans with 4 stars and 50% for plans with 3.5 stars (Determine 6). Whereas star scores don’t incorporate any measures of community breadth, they’re one of many extra salient measures out there to potential enrollees.
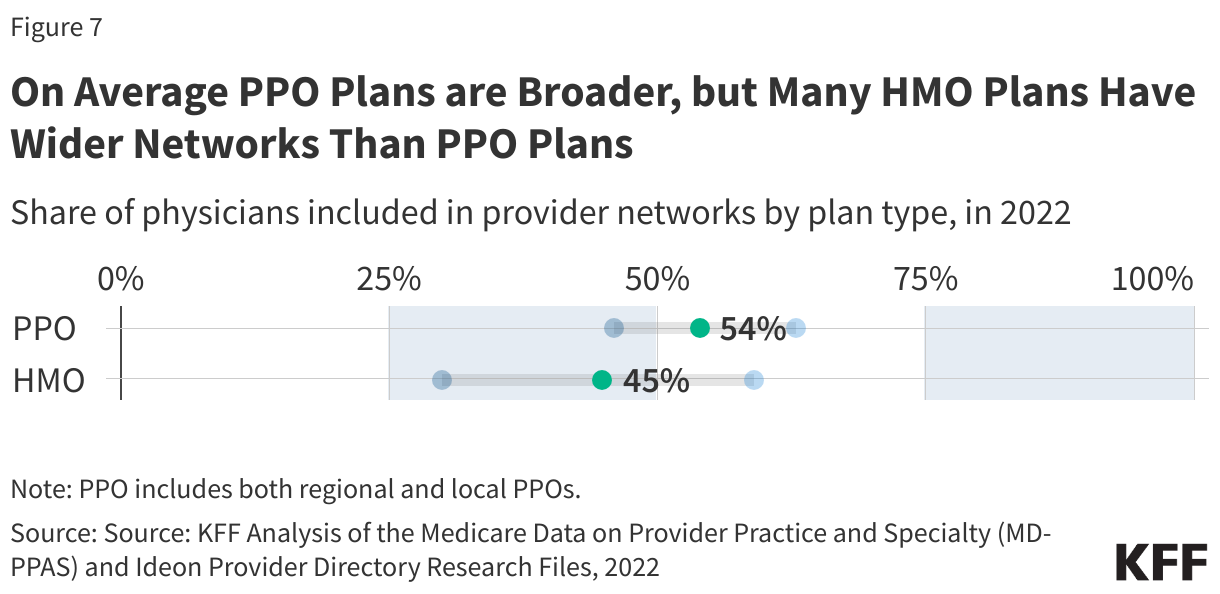
PPOs had broader doctor networks, on common, than HMOs.
In recent times, most well-liked supplier group (PPO) plans have comprised a growing share of the out there Medicare Benefit plans. For instance, between 2017 and 2025, the share of plans that had been native PPOs elevated from 24% to 43%. In 2025, greater than half of Medicare Benefit enrollees had been in HMOs. Whereas PPOs and well being upkeep organizations (HMOs) each use supplier networks, PPOs have some out-of-network protection, whereas usually HMOs don’t, besides within the case of emergencies. In 2022, simply over half (54%) of physicians out there to conventional Medicare beneficiaries had been in-network in PPO plans, on common, in contrast with 45% in HMO plans. Nonetheless, the dimensions of the networks various, significantly for HMOs, and lots of included extra physicians than the common PPO plan (Determine 7).
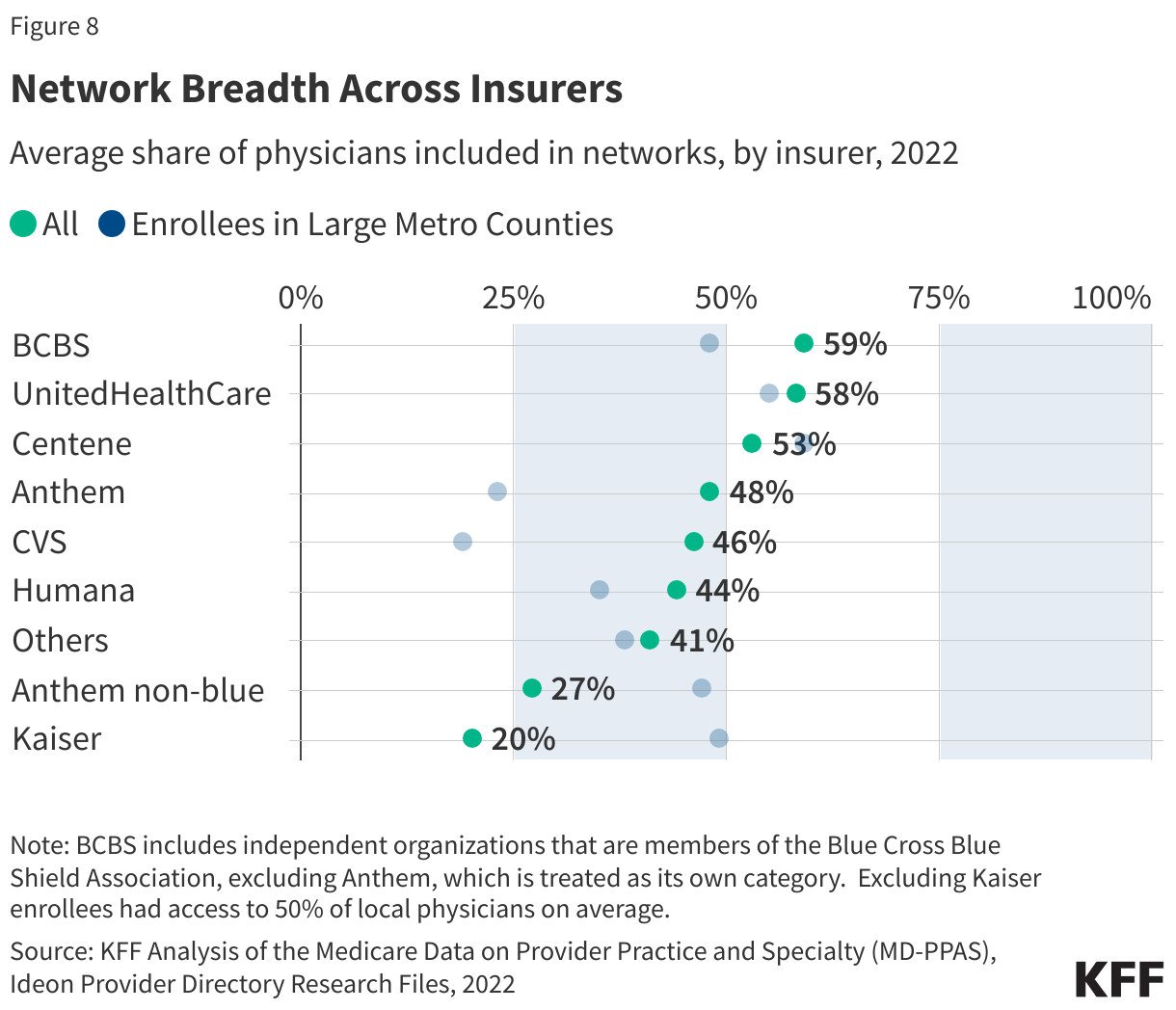
On common, Medicare Benefit plans provided by BlueCross Blue Protect associates, UnitedHealthcare, and Centene included not less than half of the physicians out there to conventional Medicare beneficiaries.
The typical share of in-network physicians various throughout Medicare Benefit insurers. Enrollees coated by UnitedHealthcare and Blue Cross Blue Protect affiliated organizations included 58% and 59% of the physicians out there to beneficiaries in conventional Medicare, respectively. Conversely, enrollees in Humana and CVS coated lower than half (44% and 46% respectively), on common (Determine 8).
On the similar time, there may be appreciable variation throughout plans provided by the identical insurer. For instance, amongst enrollees in Humana Medicare Benefit plans, 6% p.c had 25% or fewer physicians out there to conventional Medicare beneficiaries in-network, and 34% had not less than half of physicians out there to conventional Medicare beneficiaries in-network (knowledge not proven).
In lots of instances, a single insurer could supply a number of networks in the identical space. For instance, in Maricopa, AZ (Phoenix), UnitedHealthcare provided 12 plans with 12 completely different networks, starting from 37% to 61% of physicians out there to conventional Medicare beneficiaries. In Broward, FL (Fort Lauderdale) Humana provided 19 plans with three networks, starting from 26% to 44% of physicians (knowledge not proven).
The share of physicians included in Medicare Benefit networks ranged throughout specialties
CMS has community adequacy guidelines that require Medicare Benefit plans to contract with a sure variety of main care physicians, in addition to physicians with particular specialties. Most of the specialties which might be included within the community adequacy regulation take part at a better price on common than physicians with out particular necessities. Practically three-in-ten physicians who submitted a Half B declare for a standard Medicare beneficiary had been hospital-based physicians. These physicians had been much less more likely to be included in Medicare Benefit directories (21%). Hospital-based physicians could have much less incentive to take part in Medicare Benefit networks as a result of the providers they most ceaselessly present are more likely to be coated no matter community standing. For instance, emergency drugs docs had been among the many commonest sorts of docs to not take part in a Medicare Benefit community. When an individual receives emergency providers, protection of these providers just isn’t topic to community restrictions, so it might not matter that the doctor offering the service just isn’t in community.
Typically, Medicare Benefit plans included a bigger share of outpatient medical and surgical specialists topic to community adequacy guidelines than main care suppliers, with entry starting from 61% for neurology to 72% for ophthalmology on common (Determine 9). The particular specialties and distance necessities established by these guidelines are listed within the Appendix. These doctor classes don’t symbolize all physicians or specialists an enrollee might have, however spotlight a number of the key capabilities that older People typically require.
An ongoing problem in assessing community breadth is the dearth of up-to-date, dependable knowledge. As detailed within the Strategies, this evaluation has a number of limitations: it contains solely particular person physicians listed in plan directories who submitted not less than one Half B declare in the course of the yr. “Phantom” suppliers these within the listing however not really accepting the plan within the place and specialty listed, can overstate community measurement, whereas taking part suppliers lacking from directories could make networks seem narrower than they’re.
This work was supported partly by Arnold Ventures. KFF maintains full editorial management over all of its coverage evaluation, polling, and journalism actions.
Karen Pollitz, a retired Senior Fellow at KFF contributed to this evaluation.
Strategies
This evaluation mirrored the strategies utilized in How Narrow or Broad Are ACA Marketplace Physician Networks? An extended description of trimming, assigning suppliers to addresses and specialties, in addition to different knowledge sources, is on the market here.
In whole, 4,200 particular person HMO/PPO MA plans from 2022 are included, masking a complete of 20.3 million Medicare Benefit enrollees. This evaluation excludes enrollees in employer- or union-sponsored group plans in addition to Medical Financial savings Account (MSA) and Personal Payment-For-Service plans (PFFS). 11% of enrollees had been dropped from the evaluation both as a result of knowledge weren’t out there or primarily based on the trimming guidelines described within the linked strategies.
An issuer could use the identical supplier community for a number of plans, both in numerous markets or throughout the similar service space. In some areas, insurers could use a number of networks throughout the plans they provide. Plans differ in necessary respects apart from the supplier community, together with which providers are coated and the construction of cost-sharing. In whole, Medicare Benefit plans used 981 networks in 2022.
This transient considers the share of obtainable physicians round an enrollee’s house who’re listed of their plan’s community listing. Info on plan supplier directories was collected by Ideon and made publicly out there with assist from the Robert Wooden Johnson Basis. Obtainable physicians are those that follow throughout the county or are throughout the distance requirements specified within the Medicare Benefit community adequacy requirements. Thus, a wider radius is used for enrollees dwelling in additional rural counties or for specialist physicians. For instance, in a big metro county, PCPs are included if they’re throughout the county or inside 5 miles of its population-weighted middle, in comparison with 30 miles from the county middle in rural areas. A specialist, equivalent to a heart specialist, is included in giant metro counties if they’re throughout the county or 10 miles of its middle and inside 60 miles of a rural county.
Personal well being plan community directories typically embody vital numbers of “phantom” physicians who aren’t really in-network, typically as a result of they’ve retired or are in any other case now not offering care. To estimate the whole variety of physicians who’re in energetic follow, we relied on MD-PPAS, a federal database of physicians who submitted not less than one Medicare Half-B declare in 2022. This knowledge set is predicated on claims and subsequently identifies individual-level physicians who noticed not less than one Medicare affected person within the yr. Medicare Half B is the largest payer of physician services and disabled People. Nearly all non-pediatric physicians take part in this system, with about 1% formally opting out collectively. MedPac, stories that the share of clinicians who settle for Medicare is corresponding to the share that settle for personal insurance coverage. In whole, 680,000 physicians, together with 181,000 PCPs had been included in MD-PPAS in 2022. MD-PPAS categorizes physicians into 5 completely different specialists primarily based on the providers they submitted claims for; these are primary-care (26% of physicians), medical specialists (19%), surgical specialists (16%), OBGYN (5%), hospital-based specialists (29%), and psychiatrists (4%).
This transient calculates a doctor participation price, or the share of MD-PPAS physicians who had been listed in every MA listing. Whereas this methodology ensures that physicians who aren’t working in any respect, aren’t included within the evaluation, networks should embody “phantom” suppliers who’re actively training however who’re inaccurately listed as taking part within the plan. Additional, this evaluation doesn’t contemplate whether or not the doctor is presently seeing sufferers or for which providers they’re in-network. Conversely, solely physicians enumerated within the listing are included. As defined within the linked strategies, physicians related to group practices, physicians working exterior of their main addresses, and others could also be excluded.
Info on plan kind, star scores, plan enrollmen,t and plan traits was collected from CMS in a way described here and here. Info of the demographic traits of enrollees was collected from the Grasp Beneficiary Abstract File (MBSF), 2022. Info on county traits was obtained from the 2020 CDC/ATSDR Social Vulnerability Index. Knowledge on doctor provide in counties was obtained from the Space Useful resource File (ARF) 2022.
Appendix
Medicare Benefit plans are typically required to incorporate a minimal variety of suppliers throughout varied specialties and facility classes. Inside Medicare Benefit community adequacy requirements, plans should embody a tiny fraction of the suppliers working in or close to the county. These rules act as a ground and grant plans appreciable latitude. This transient considers the share of obtainable physicians round an enrollee’s house who’re listed of their plan’s community listing. Obtainable physicians are those that follow throughout the county or are throughout the distance requirements specified within the Medicare Benefit community adequacy requirements (Desk 1).
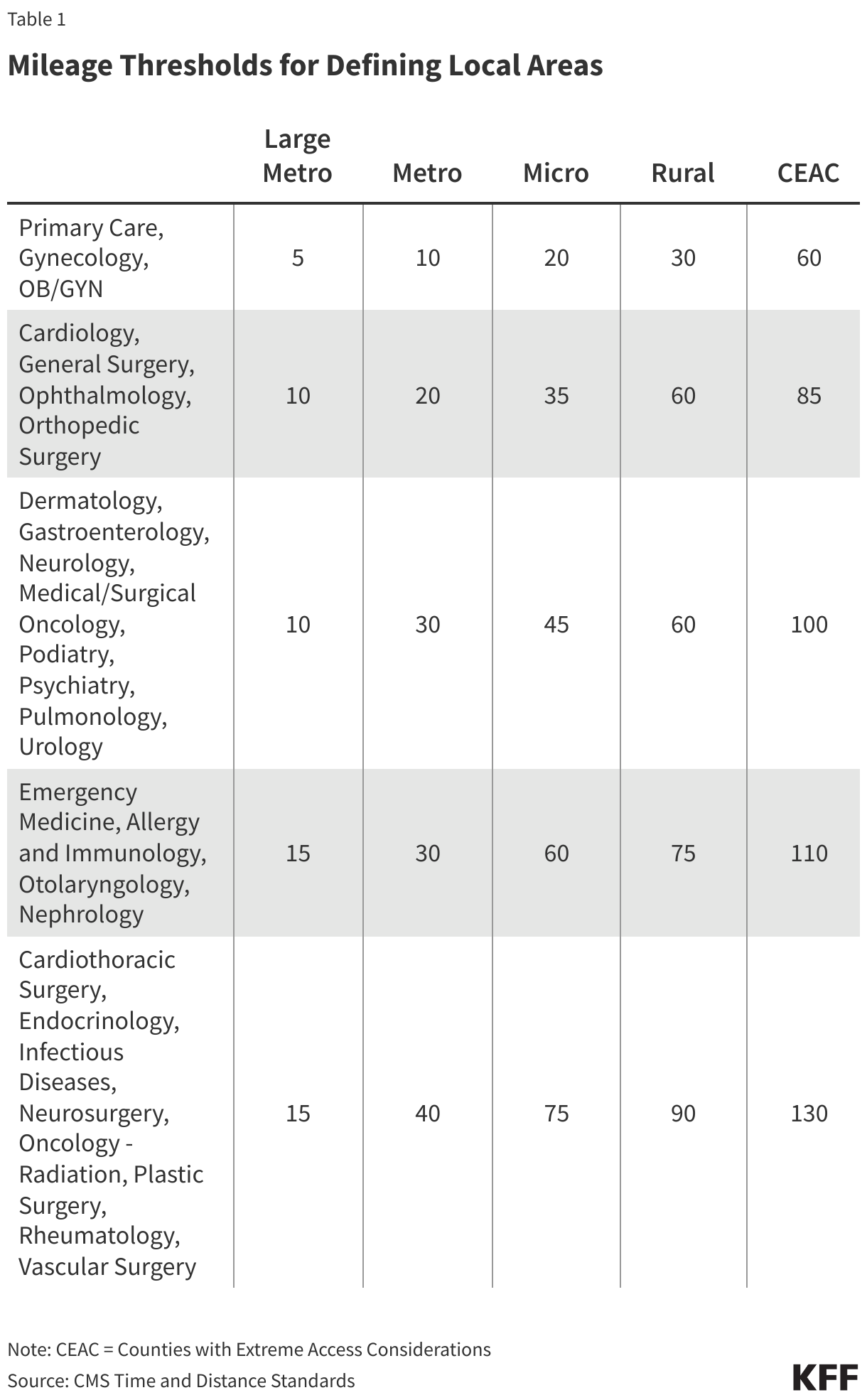
In whole, CMS designates 78 “Giant Metro” counties primarily based on their inhabitants and inhabitants density, and 720 “Metro” counties. For instance, Giant Metro areas are categorised as counties with not less than 1,000,000 folks and a inhabitants density of not less than 1,000 folks per sq. mile, or counties with between 500,000 to 999,999 folks and a inhabitants density of not less than 1,500 folks per sq. mile, or counties with a inhabitants density of not less than 5,000 folks. The county classifications comply with the definitions used within the Medicare Benefit community adequacy guidelines (Table 3-1). Most Medicare Benefit enrollees reside in one in every of these city county-designations, together with 29% in “Giant Metro” counties and 53% in “Metro” counties.