
Over one-third of Medicaid spending pays for long-term care, with a lot of the spending paying for residence care—often known as “home- and community-based providers” or HCBS. Medicaid pays for nearly 70% of all home care spending within the U.S., almost all of which is supplied by optionally available providers. Amongst these optionally available providers, states rely closely on Medicaid “waivers” to offer residence care, which permit them to handle prices utilizing mechanisms comparable to capping spending or enrollment within the waiver (Field 1). States can also use ready lists to trace and handle individuals who need to obtain however usually are not but receiving residence care. Whereas ready lists could end result from caps on waiver spending or enrollment, states additionally used them for different administrative causes (Field 2).
Medicaid’s vital spending on residence care and the supply of mechanisms for limiting such spending might spur states to chop residence care spending in response to the 2025 reconciliation law. Reducing spending on residence care might lead to both fewer folks receiving any advantages or folks receiving fewer lined providers, despite the fact that the necessity for residence care is unlikely to fall in future years. The lately handed reconciliation legislation is estimated to scale back federal Medicaid spending by $911 billion between 2025 and 2034, roughly a 14% discount in federal funding for this system. Over the past main discount in federal Medicaid spending, all states reduced spending on residence care by serving fewer folks (40 states) or by chopping advantages or fee charges for long-term care suppliers (47 states).
Utilizing knowledge from the 23rd KFF survey of officials administering Medicaid residence care applications, this challenge transient describes the mechanisms states are at present utilizing to restrict Medicaid spending on residence care and their plans for adopting new mechanisms in state fiscal yr (FY) 2026. The survey was despatched to all residence care applications in all 50 states and the District of Columbia (hereafter known as a state), which states accomplished between April and July 2025. All states besides Florida accomplished the survey, though response charges for particular questions could have been decrease. States typically accomplished the survey previous to enactment of the reconciliation legislation, so modifications to restrict spending in FY 2026 usually are not attributable to the brand new legislation. Survey findings are reported by state and waiver goal inhabitants, though states typically provide a number of waivers for a given goal inhabitants. Key takeaways embody:
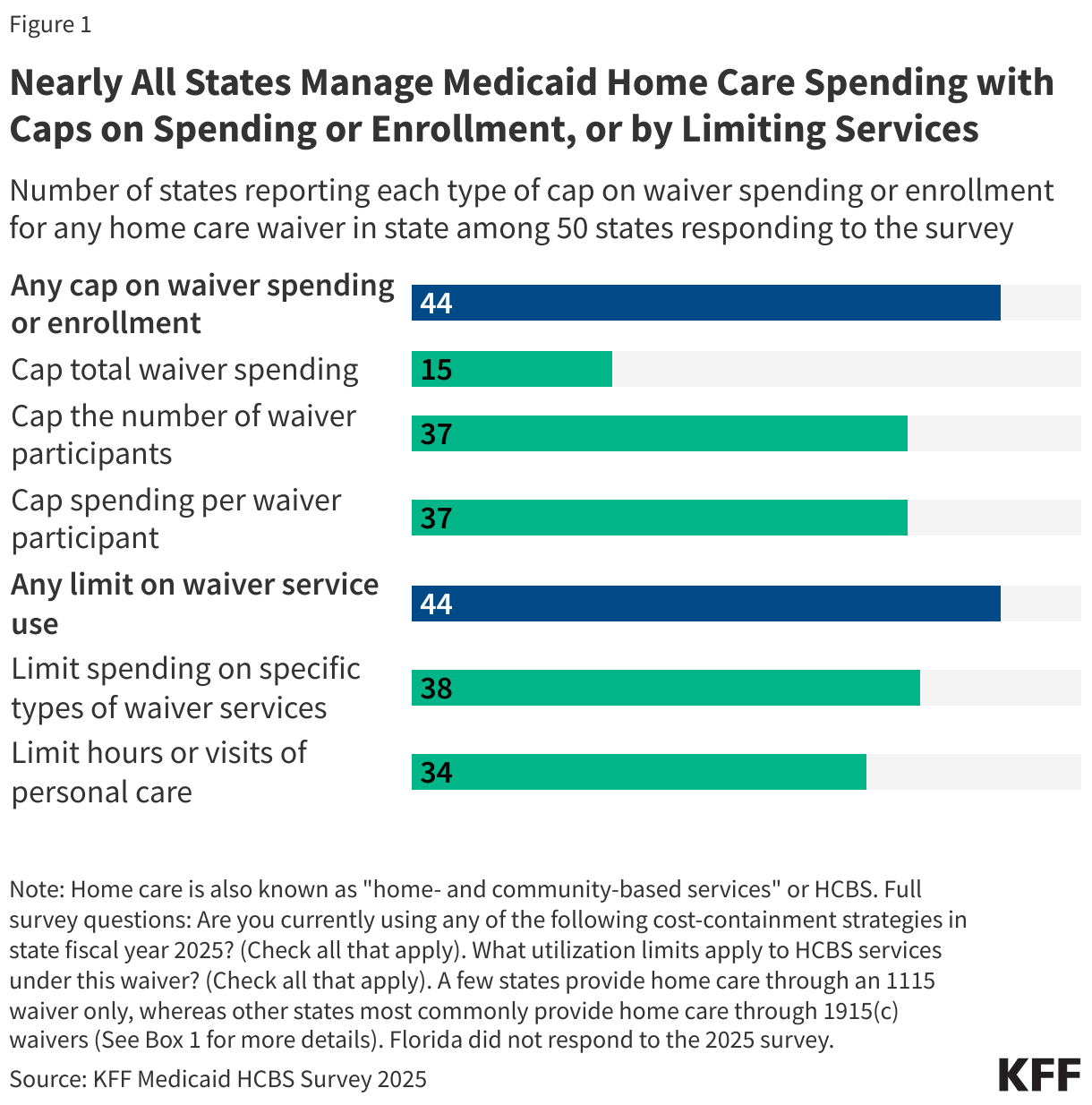
- For many residence care providers, that are delivered by waiver applications, 44 out of the 50 responding states constrain spending by limits on both complete enrollment (37 states) or on complete spending (15 states, Determine 1). Most states (37) additionally cap waiver spending per participant for at the least one waiver.
- Most states (44) reported utilizing mechanisms in at the least one waiver to restrain spending that applies to particular providers, comparable to limiting the quantity of spending for providers per participant (38 states) or limiting the amount of non-public care enrollees could obtain (34 states).
- Almost a 3rd of responding states (15) reported planning to undertake new methods in FY 2026 to comprise residence care prices. Since most survey responses had been collected earlier than enactment of the reconciliation invoice, it isn’t but identified how this quantity will change as states put together for the forthcoming cuts to federal Medicaid spending.
- Fewer mechanisms can be found to states in managing spending for residence care providers supplied exterior of waivers, however almost all states use prior authorization as a device to handle that sort of spending.
Field 1: Authorized Necessities and Choices for Medicaid Dwelling Care Waivers
Most Medicaid residence care is supplied by 1915(c) waivers, which permit states to offer residence care to individuals who choose to obtain long-term care of their residence or group reasonably than from an establishment. The 1915(c) waiver permits states to waive a number of necessities of Medicaid legislation together with that providers be accessible statewide, and on a comparable foundation to all Medicaid enrollees. States could provide quite a lot of limitless providers by the waiver, and states tailor the profit packages to satisfy the wants of a specific goal group. All providers should comply with an individualized plan of care. Amongst different necessities, 1915(c) waivers should display that the providers is not going to price greater than institutional care would. This requirement is carried out by a cost neutrality test [see Instructions, Technical Guide and Review Criteria V3.7], that compares the per particular person prices of waiver providers to the per particular person prices of offering care to related folks in an institutional setting.
States are permitted, however not required, to set limits on complete enrollment or spending in a 1915(c) waiver. Enrollment limits could take a number of kinds together with the variety of members served, the variety of enrollees at a given time, or the speed at which individuals are enrolled or disenrolled. States can also hold waiver slots accessible as “reserve capability” for folks to enroll on a precedence foundation, comparable to folks transitioning from establishments to the group or folks in disaster.
4 states additionally solely present residence care by 1115 waivers, which supply states an avenue to check new approaches in Medicaid that differ from what’s required from federal statute, if the method is more likely to “promote the targets of the Medicaid program” within the view of the Secretary of Well being and Human Providers. There isn’t a statutory requirement for waivers to be “price range impartial,” however long-standing coverage and apply has required states to display price range neutrality. One option to display price range neutrality is to point out that per enrollee spending over the course of the waiver doesn’t exceed projected per enrollee spending within the absence of the waiver.
Mechanisms for Limiting Waiver Dwelling Care Spending and Enrollment
Most states (37) handle Medicaid spending on residence care by capping both complete enrollment, or each complete spending and enrollment (Determine 1). Most states additionally cap per particular person spending for residence care waiver providers. The 2 major sorts of waivers states use to supply Medicaid home care are 1915(c) and 1115. The 2 waivers differ in that 1915(c) waivers are particularly used to offer Medicaid residence care to individuals who require an institutional degree of care whereas 1115 waivers can check all sorts of new Medicaid approaches (Field 1). Among the many 50 responding states that present residence care by waivers, 15 states have caps on complete waiver spending, 37 have caps on the whole variety of members, and 37 have caps on spending per particular person (Appendix Desk 1).
Field 2: Variations Between Waiver Caps and Ready Lists
Though caps on complete spending or members could lead to ready lists when the caps lead to too few waiver slots relative to the quantity of people that want to obtain providers, in lots of circumstances, ready lists and enrollment caps are conceptually totally different. In almost all states, there are waivers that use spending or enrollment caps however don’t have ready lists or waivers which have ready lists with out spending or enrollment caps.
States could constrain waiver spending by capping complete enrollment or complete spending however not have a ready checklist for that waiver within the following sorts of conditions:
- The caps are set excessive sufficient that no individuals who want to obtain providers are unable to take action,
- The state permits all candidates to enroll within the waiver however limits spending by decreasing the providers supplied, or
- The state allocates providers to folks with the best want and refers people who find themselves not authorized for waiver providers to different residence care applications.
States could have ready lists within the absence of caps on enrollment or complete spending within the following sorts of conditions:
- Folks have registered to obtain residence care, however the state has not but decided whether or not they’re eligible,
- Persons are decided eligible for waiver providers, however they haven’t but had their degree of care assessed or began receiving providers, or
- Persons are eligible for providers however not receiving them on account of supplier shortages.
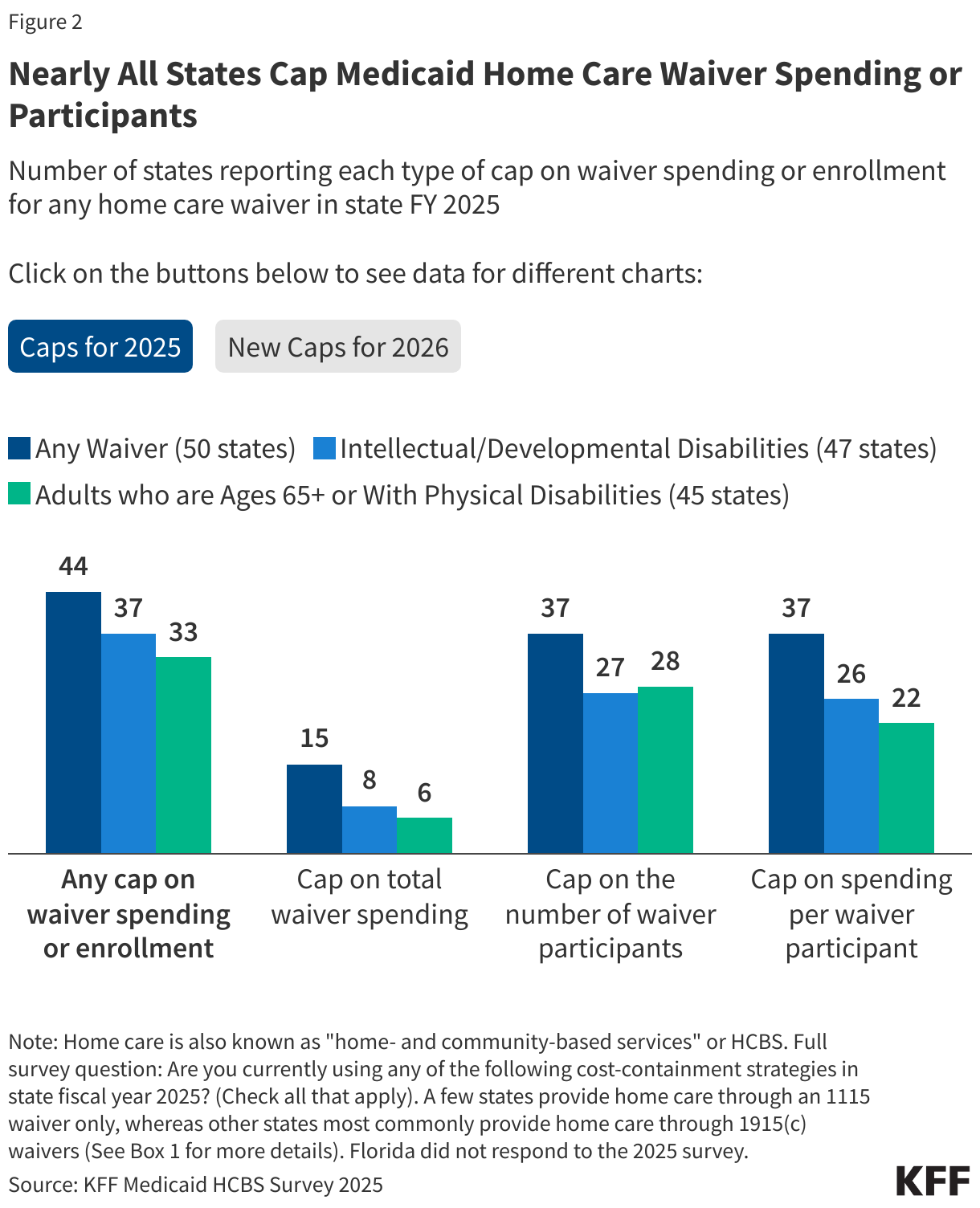
Use of caps on complete spending, participation, or prices per participant had been reported in 44 states (Determine 2). Among the many 50 responding states with waivers, 44 had caps of some type, together with 15 with caps on complete spending, 37 with caps on complete members and 37 with caps on spending per participant. For each 1915(c) and 1115 waivers, states are required to satisfy price neutrality necessities to display that the prices per enrollee in waiver providers don’t exceed the per enrollee prices of institutional care (Field 1). States could meet this requirement by exhibiting that common prices per enrollee are under the common prices of institutional care or they could set up price limits for all members enrolled within the waiver. States that undertake such individual cost limits [see Instructions, Technical Guide and Review Criteria V3.7] should specify the safeguards in place to deal with folks’s wants after they’ve reached the person price restrict.
Use of caps is comparable for waivers that serve totally different goal populations. Amongst waivers for folks with mental or developmental disabilities (47 states) or people who find themselves ages 65 and older or have bodily disabilities (45 states), the variety of states with caps on complete spending (8 and 6 respectively), participation (27 and 28), and spending per participant (26 and 22) are related. Comparable developments additionally apply for waivers which might be accessible in a smaller variety of states (Appendix Desk 2).
Lower than 1 / 4 of states (11) reported planning to undertake new mechanisms to restrict waiver enrollment or spending in state FY 2026. Amongst states which might be planning to undertake new mechanisms, caps on the variety of waiver members are commonest (8 states) with few states planning to newly cap spending per waiver participant (4) or complete waiver spending (1). Solely two states, Maryland and Oregon, reported planning to undertake multiple mechanism (Appendix Desk 4).
Mechanisms for Limiting the Prices of Particular Waiver Dwelling Care Providers
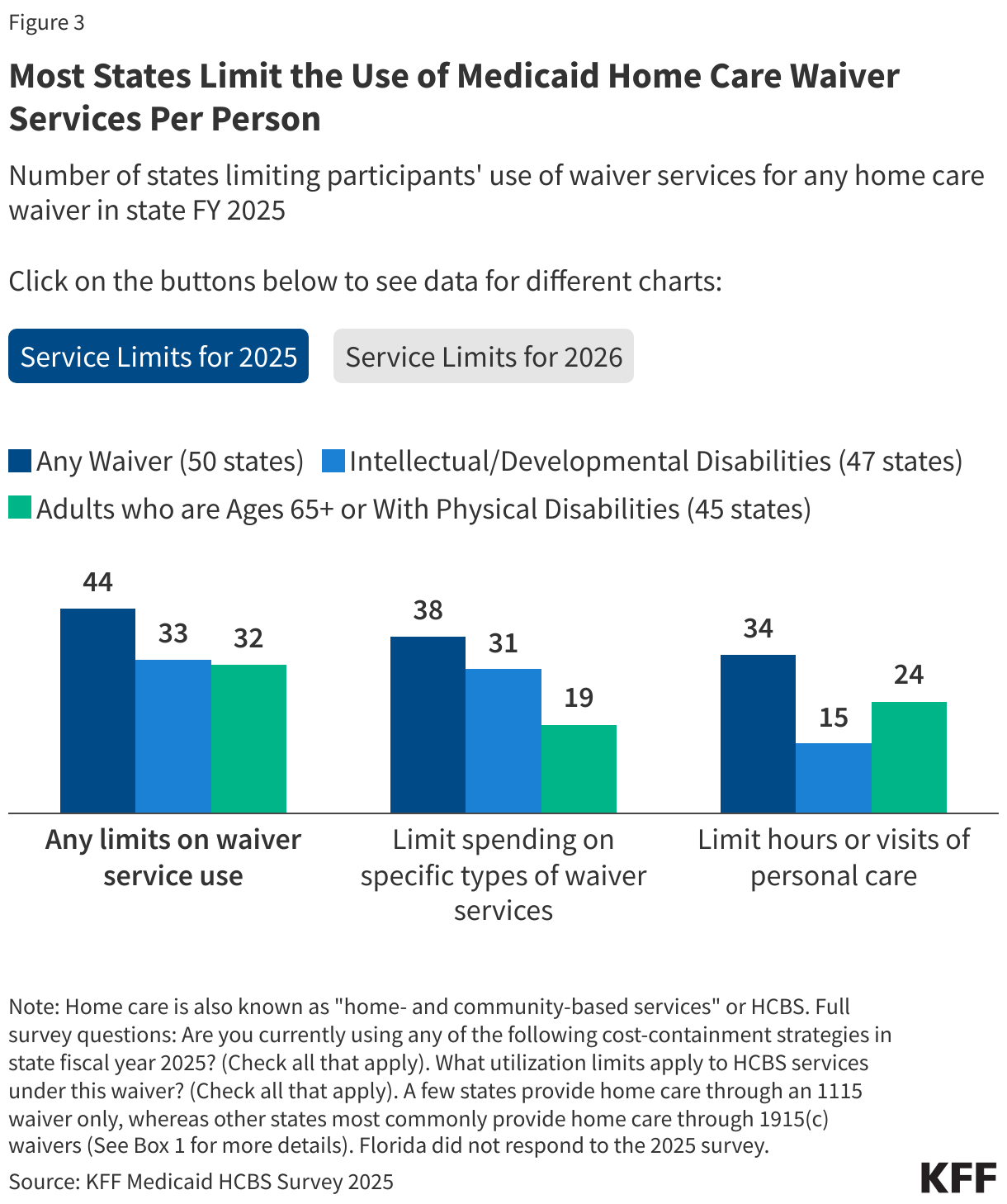
Most states (44) use at the least one mechanism to constrain the prices of particular residence care providers per participant of their waivers (Determine 3). Amongst states with service-specific limits, caps on spending for particular providers (38 states) are extra widespread than volume-based limits comparable to most hours of non-public care or variety of visits (utilized by 34 states).
States are extra doubtless to make use of spending caps for waivers that serve folks with mental and developmental disabilities however are extra doubtless to make use of volume-based limits for waivers that serve older adults and other people with bodily disabilities. Of the 47 states providing 1915(c) waivers serving folks with mental and developmental disabilities, near two-thirds of states (31) cap spending for waiver providers per participant and almost a 3rd restrict private care hours or visits per particular person (15 states). For the 45 states with waivers serving people who find themselves ages 65 and older or have bodily disabilities, limits on the amount of non-public care are extra widespread (24 states) than caps on spending for waiver providers per participant (19 states). The variety of states with these service caps varies for much less widespread waivers. The utmost variety of hours or visits of non-public care differ by state and over a 3rd of states decide limits by a useful evaluation (19 states).
States reported capping spending on a variety of various waiver providers, together with residence and automobile accessibility modifications and adaptive tools and assistive know-how. Dwelling and automobile accessibility modification limits, comparable to ramps and wheelchair van lifts, differ throughout states; Delaware and Nebraska have waivers serving folks with mental and developmental disabilities that cap diversifications to $10,000 per participant each 5 years whereas Massachusetts waivers for a similar inhabitants restrict residence modifications to $50,000 and automobile modifications to $25,000 per participant in a five-year interval. Some states, like Illinois, group all tools, know-how, and modifications right into a mixed class for spending limitations, however different states have separate caps. For instance, Louisiana’s waiver serving folks with mental and developmental disabilities caps spending on specialised medical tools at $2,500 per yr and Michigan’s waiver for people who find themselves ages 65 and older or have bodily disabilities caps spending on assistive know-how at $5,000 per yr.
For FY 2026, 12 states reported planning to undertake new waiver service limits to constrain prices. New caps on spending for particular sorts of waiver providers per participant (8 states) are extra widespread than limits on the amount of non-public care (5 states). Connecticut is the one state that reported planning to undertake each mechanisms (Appendix Desk 4).
Use of Prior Authorization to Handle Spending on State Plan Dwelling Care
For Medicaid residence care that’s supplied by the state plan, states can’t use waiver-specific mechanisms for constraining prices however do typically use prior authorization. State Medicaid businesses typically require enrollees to acquire approval of sure well being care providers or drugs earlier than the care is supplied—an insurance coverage apply generally known as “prior authorization.” In Medicaid, prior authorization is used for each obligatory providers, comparable to residence well being, and optionally available providers, comparable to private care, and is broadly utilized by Medicaid managed care organizations. If the requested service is deemed not applicable or medically crucial, the request could also be denied (absolutely or partially), however enrollees could possibly enchantment the choice by sure appeals and exemption procedures. Nonetheless, the appeals course of will be troublesome to navigate, and people could also be denied entry to wanted care whereas ready for a choice. In a KFF survey carried out in July 2025, 79% of Medicaid enrollees underneath age 65 and 67% of these ages 65 and older discovered delays and denials of well being care providers by medical health insurance corporations to be a serious downside.
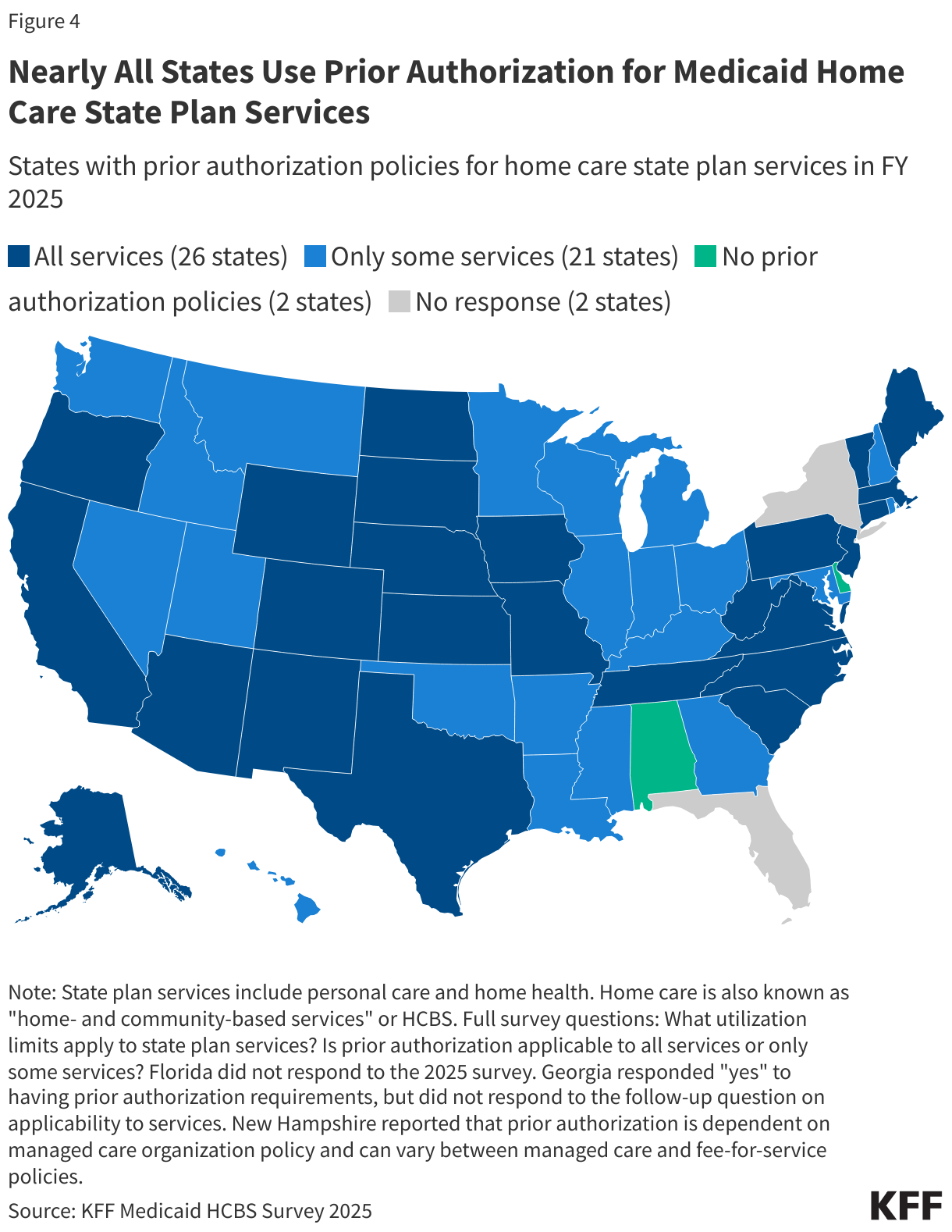
Almost all states (47) reported utilizing prior authorization to constrain prices on both private care or residence well being providers (Determine 4). Amongst these states, over half (26) use prior authorization for all residence care providers, whereas the remaining states (21) have this coverage in place for just some providers. Dwelling well being is a compulsory profit for all states, and 40 states use prior authorization for residence well being. Private care is an optionally available profit supplied by 33 states, and almost all (29) use prior authorization for private care. Frequent providers that require prior authorization embody private care, personal obligation nursing, specialised tools and know-how, and residential and automobile modifications. Prior authorization can be used for residence care service requests above sure thresholds (e.g. greater than 40 hours per week of non-public care).
States reported that prior authorization for Medicaid residence care providers could also be carried out by varied entities, together with Medicaid businesses, different state entities, managed care organizations, or case managers. Throughout state plan providers, the commonest entities accountable for approving or denying providers are managed care organizations (12 states), utilization administration distributors (7 states), state Medicaid businesses (6 states), or different state businesses (6 states). The identical entities are sometimes accountable for conducting prior authorization for waiver providers.
States can also use prior authorization for waiver providers, however it might be a part of person-centered service planning necessities that apply to all 1915(c) waivers [see Instructions, Technical Guide and Review Criteria V3.7]. All providers supplied by a 1915(c) waiver should be specified prematurely by a written service plan, often known as a plan of care. The plan is meant to offer a whole image of how enrollees’ wants are met. The plan paperwork which particular waiver providers shall be supplied to members, together with the quantity, period, and frequency of every service, and the sorts of suppliers that will furnish every service.
KFF requested states about whether or not they required price sharing for residence care and located that few do. Solely 3 states reported requiring price sharing for private care supplied by waivers (Georgia, Illinois, and Rhode Island) and three states reported requiring copayments for different waiver providers (Minnesota, Oklahoma, and Rhode Island). Moreover, 3 states (Georgia, Idaho, and Maine) reported requiring copayments for residence well being providers. No states reported adopting new copayments for state FY 2026. Beginning October 1, 2028, the reconciliation legislation requires states to impose price sharing of as much as $35 per service on adults eligible for Medicaid by the Reasonably priced Care Act Medicaid growth with incomes 100-135% FPL. Almost 400,000 Medicaid enrollees who use long-term care are eligible on account of the Medicaid growth, and that group shall be required to pay price sharing underneath this requirement. It’s unknown whether or not states will select to use the associated fee sharing necessities for residence care extra broadly—both on account of administrative efficiencies or as a mechanism to scale back state spending on residence care in response to the historic discount in federal Medicaid funding from the reconciliation legislation.
This work was supported partly by Arnold Ventures. KFF maintains full editorial management over all of its coverage evaluation, polling, and journalism actions.